Lower back pain and pelvic girdle pain (PGP) are common conditions in pregnancy, with an estimated incidence of 4–84%.1 The variability in incidence is due to ambiguity in definitions and diagnostic criteria. Pain is not limited to a particular trimester during pregnancy but is often experienced throughout pregnancy and postpartum; however, the onset is usually at 14–30 weeks gestation.2
There have been many terms used to describe lower back and pelvic pain in pregnancy (eg ‘pelvic instability’, ‘lower back pain’ and ‘symphysis pubis dysfunction’).3 The 2005 European guidelines describe two common patterns of pain: PGP and lumbar pain. 4–6 Lumbar pain is defined as pain experienced in the region between the last thoracic spinous process and first sacral spinous process, laterally bound by the lateral borders of the lumbar erector spine.4,7 The focus of this article will be PGP in pregnancy.
Many clinicians do not regard PGP as a serious complication of pregnancy and an Australian study found that only 25% of women who reported PGP were offered any treatment.3
Pelvic girdle pain
PGP is defined as pain between the posterior iliac crest and the gluteal fold, particularly in the vicinity of the sacroiliac joint (SIJ), which may radiate to the thighs and hips. PGP can occur in conjunction with or separately to pain in the pubic symphysis.4–7 There is diminished capacity for activities such as standing, walking and sitting, and the pain or functional disturbance is reproducible by specific clinical tests.6
PGP results in greater disability than lumbar pain and is more prevalent in pregnant women.8 PGP can result in significant physical disability and has important psychosocial implications, including extended leave from work during pregnancy, poorer quality of life (as a result of being unable to carry out normal roles, affecting their ability to care for their children) and predisposition to chronic pain syndrome.3,7,9
Aetiology and pathophysiology
The development of PGP in pregnancy is multifactorial and is related to hormonal, biomechanical, traumatic, metabolic, genetic and degenerative factors.1,7,10
Suggested biomechanical pathophysiology focuses on an already maximally stressed lumbar spine secondary to the enlarging uterus.7 There is a shift in the maternal centre of gravity that transfers force onto the lumbar spine, causing stress in the lower back and pelvic girdle, and resulting in compensatory postural changes such as increased lumbar lordosis.7,8,10 Women with PGP have increased pelvic, thoracic and lumbar joint mobility, resulting in pelvic instability and pain.11 Lumbopelvic muscle strength and coordination are reduced as a result of altered mechanical forces at the pelvic girdle.7
The importance of hormonal influences in PGP is unclear. While the hormone relaxin in pregnancy is often associated with joint laxity, there is no clear correlation between serum relaxin levels and peripheral joint laxity or PGP.7,10
Risk factors for PGP
Women with previous pelvic or lower back pain in and/or out of pregnancy and/or a history of trauma to the back or pelvis have an increased risk of developing PGP.1,3,10 Multiparity, increased body mass index, physically demanding work, emotional distress and smoking also increase a woman’s risk.1,6,7,12,13 However, age, hormonal contraceptive use, height, weight and time interval since last pregnancy are not risk factors for PGP.1,6,10,12
Assessment
A detailed history and physical examination, including specific diagnostic tests, can aid in timely and accurate diagnosis of PGP.
6,7,10 PGP in pregnancy is diagnosed after exclusion of other significant pathologies and/or obstetric complications (Table 1).
1,6,7
|
Table 1. Differential diagnosis of pelvic girdle pain in pregnancy6,7
|
|
Orthopaedic/musculoskeletal
|
Obstetric and gynaecological
Infective
-
Urinary tract infection
-
Osteomyelitis
Vascular
|
History
A thorough history, including an obstetric and pain history, is essential in assessing a pregnant patient presenting with pelvic pain. It is important to determine if the pain is mechanical in nature – that is, associated with activity and eases with rest – as pain that arises in the absence of mechanical stimuli is unlikely to be PGP. Initial history will also identify ‘red flags’ of possible serious pathology (Box 1).11
|
Box 1. Red flag history points6,10
|
-
Pain in the absence of mechanical stimuli
-
Unexplained weight loss
-
Neurological symptoms: saddle paraesthesia, acute onset radicular pain with associated numbness, weakness or paralysis
-
Incontinence or bladder and bowel dysfunction
-
Significant trauma history (eg fall from height, heavy lifting)
-
Vaginal bleeding/fluid loss
-
Pyrexia of unknown origin
|
Examination
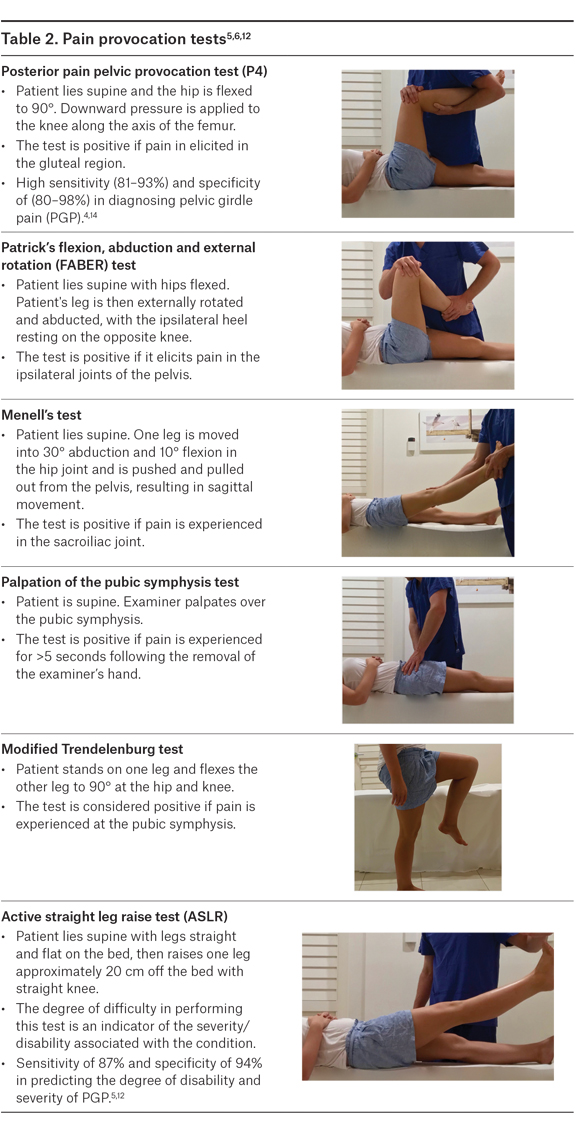
PGP is diagnosed on the basis of the site of pain and the ability to reproduce the pain using specific provocation tests (Table 2).6,7,14 There is no gold standard clinical test, but the posterior pain pelvic provocation test (P4), Patrick’s flexion, abduction and external rotation (FABER) test and Menell’s test are of greatest theoretical and empirical relevance for SIJ pain. The palpation of the symphysis test and modified Trendelenburg’s test are the most sensitive and specific for symphysis pubis pain.6,14
.jpg.aspx "AJGP-07-2018-Focus-Nippita-Pelvic-Pain-Table-2-(1).jpg")
Investigations
Investigations are not an integral part of diagnosing PGP because the diagnosis is clinical; however, investigations may be helpful if there is concern about more complicated differential diagnoses. Imaging should be used judicially after a thorough clinical assessment, especially as there are ongoing concerns regarding the effects of ionising radiation exposure on the fetus. Imaging does not aid in assessing the severity of PGP and should only be used in rare cases.6–8 Indications for imaging include, but are not limited to, persisting non-mechanical pelvic pain, severe mechanical pain that is not responding to appropriate management, an inability to weight-bear, clinical suspicion of sinister pathology or presence of any red flags described in Box 1.6 Plain pelvic X-rays can assist in measuring the degree of symphyseal separation and identifying cortical abnormalities such as sclerosis and rarefaction if suspected.10 There is no increased risk to the fetus with the radiation dose received from a single plain pelvic film.15 Magnetic resonance imaging is supported for the investigation of differentials for PGP, with the added advantage of increased resolution and superiority of visualisation of soft tissue/marrow with no exposure to ionising radiation.6,10
Management
PGP is managed conservatively by a multidisciplinary team. Management includes addressing the psychosocial implications for the woman and her family.1,10 However, the National Health and Medical Research Council antenatal care guidelines on management of PGP found limited high-quality evidence to recommend specific clinical practices.1 A strategic approach should be implemented for activity modification, pelvic support garments, management of acute exacerbations, physiotherapy and exercise programs to prevent progression of symptoms, and referral.6,11
Activity modification involves identifying the aggravating activities and developing strategies to avoid them. The majority of aggravating activities involve unilateral weight-bearing or shearing forces through the pelvis.6,7,11 Even simple daily activities such as getting dressed can place uneven stress on joints, and sitting to avoid single leg stance is recommended (Box 2).10
|
Box 2. National Health and Medical Research Council (NHMRC) antenatal care guidelines – Practical advice for minimising pain1
|
-
Wearing low-heeled shoes
-
Seeking advice from a physiotherapist regarding exercise and posture
-
Reducing non-essential weight bearing activities (eg climbing stairs, standing/walking for long periods of time)
-
Avoiding standing on one leg (eg by sitting down to get dressed)
-
Avoiding movements involving hip abduction (eg getting in/out of cars, baths or squatting)
-
Applying heat to painful areas
|
|
Reproduced with permission from Homer C, Oats J. Clinical practice guidelines: Pregnancy care. Canberra: Australian Government Department of Health, 2018; p. 355–57.
|
Pelvic support garments can provide stabilisation at the pelvic girdle and reduce pain and severity of symptoms if fitted correctly and used for short periods of time.6
Management of acute exacerbations may involve a short period of bed rest with appropriate use of analgesia.10 Simple analgesia such as paracetamol and low-potency opioids can be considered; however, opioids need to be used cautiously because of side effects and the potential for dependence and neonatal withdrawal.16 Given the increased risk of thrombosis, pregnant women on bed rest should be offered prophylactic dose low molecular weight heparin. There is limited evidence that acupuncture given in addition to standard treatment is more effective in relieving PGP than standard treatment or physiotherapy alone.6,17 However, women have reported a reduction of morning and evening pain and improved functional outcomes with acupuncture.1
Physiotherapy and specific exercise programs provide benefit by reducing the severity of acute exacerbations and promoting correction of the underlying mechanical adaptations and deficits.6 Targeted exercises promote strength of the gluteal and adductor muscles in conjunction with reduction of the activity of lumbar spine musculature.6,10,16 Physiotherapists can also provide management strategies to reduce the impact of unavoidable daily living activities that cause aggravation of symptoms.
Surgical management is rarely considered and only after all non-invasive measures have failed and there are persistent debilitating symptoms.10 External stabilisation devices are trialled prior to surgery to determine if mechanical instability is the cause of pain and relieved with fixation.6
When to refer
Referral to appropriate specialist services is indicated with the presence of any red flag symptoms (Box 1). Neurological deficits are not a normal feature of PGP and should be promptly referred for further investigation and management.1,7 Refractory pain that is not reduced or able to be managed using the methods outlined in the management described above can necessitate referral to a pain service. Appropriate use of a specialist pain service may reduce the risk of developing a chronic pain syndrome and/or facilitate further investigation into the cause of pain.6 Three serious conditions associated with pelvic pain in pregnancy – transient osteoporosis of pregnancy, osteonecrosis of the hip and pubic symphysis diastasis – require referral to specialist services and are discussed in Appendix 1.
Prognosis and recurrence risk
The outcomes for women with PGP in pregnancy are good, with 93% of women reporting symptomatic resolution within three months postpartum.10 However, PGP frequently recurs in subsequent pregnancies, and increasing the interval between pregnancies does not change the recurrence risk or severity of subsequent PGP.16 In one study, 68% of multiparous women reported recurrence of PGP, and 70% of these women reported PGP being worse in the subsequent pregnancy.18
Conclusion
Although PGP is common, it can adversely affect the woman’s quality of life and daily activities. Simple practical recommendations, such as wearing low-heeled shoes, reducing non-essential weight-bearing activities and avoiding movements that require hip abduction, will help minimise disruption to the woman. General practitioners are an integral part of the multidisciplinary team in setting the course for the woman’s experience, management and treatment of PGP.
|
Appendix 1. Important orthopaedic differential diagnoses of pelvic girdle pain
|
|
Transient osteoporosis of pregnancy usually occurs in the third trimester of pregnancy and usually affects a single hip. The cause is an exaggerated physiological hormonal response in pregnancy or unmasking of existing osteoporosis. Risk factors are low body mass index, primiparity, reduced calcium intake and a family history of osteoporosis. Transient osteoporosis of pregnancy presents as severe acute unilateral groin pain. Diagnosis is confirmed by magnetic resonance imaging (MRI), and the condition can be complicated by occult fractures. If clinical suspicion is high, an MRI and prompt referral should be arranged.7, 12
Osteonecrosis in pregnancy (avascular necrosis of the hip) is very rare in pregnancy and is a progressive condition with symptoms relating to the degeneration of the articular surface. The presenting symptom is increasing pain felt deep in the groin that is exacerbated by certain movements. The aetiology is speculative but may relate to the increase in unbound hormones in late pregnancy or change in mechanical forces applied to the joint with the development of a gravid uterus.6,7 Specialist orthopaedic advice is required for management of this condition.
Pubic symphysis diastasis is a rare but serious condition in pregnancy, caused by rupture and separation of the pubic symphysis. The aetiology is unclear, but risk factors are multiparity and macrosomia. Rupture is diagnosed in women with a pubic symphysis gap of >1 cm, which may be clinically palpable. Imaging gives a definitive diagnosis.6 Conservative measures including bed rest, analgesics and a pelvic binder, are effective in most cases. Referral to an orthopaedic surgeon is required for pain that does not resolve or worsens or a pubic symphysis gap of ≥4 cm.7
|