Case
A woman aged 67 years with a history of childhood tonsillectomy presented with complaints of a severe sore throat and pain on swallowing. She had not been not feeling well since the beginning of the week, and by the middle of the week her throat was sore and red. She was initially diagnosed with tonsillitis of post-surgical tonsillar remnants and prescribed cephalexin. Her symptoms had progressively worsened by the end of the week, with pain extending to the left jaw and ear, and with swallowing.
On examination, her body temperature was 37.5°C, pulse was 90 bpm and regular, blood pressure was 122/80 mmHg and oxygen saturation on pulse oximeter was 97% on room air. The airway was clear and she was breathing without difficulty.
Examination of the throat revealed vesicles extending from the left side of the soft palate to the tonsillar pillar and beyond (Figure 1). The uvula was central in position and movements of the soft palate were normal. The affected area of the throat was tender to touch (during swab collection), very sensitive to cold water and had an altered sense of taste to chocolate. The cervical lymph nodes were enlarged on the left side. There was no tragus, mastoid or temporomandibular joint tenderness present. The ear canal and tympanic membrane examination were normal.
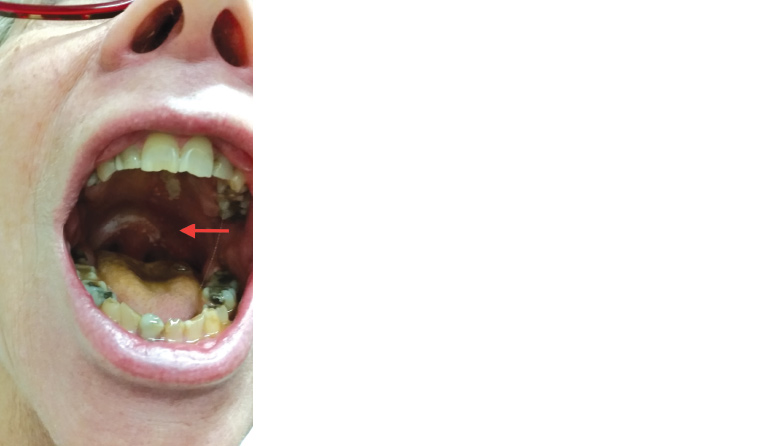
Figure 1. Vesicular lesions on the left side of the soft palate
Question 1
What is the most likely diagnosis?
Question 2
What is the pathogenesis of herpes zoster (shingles)?
Question 3
What tests can be performed by the clinician to confirm the diagnosis?
Question 4
What nerves are typically involved in herpes zoster?
Question 5
What is the significance of Centor criteria?
Answer 1
Herpes zoster involving the left glossopharyngeal nerve is the most likely diagnosis. The presence of signs restricted to the area of distribution of an isolated nerve is the classic presentation of varicella-zoster virus (VZV) reactivation. Severe pain,1 unilateral taste impairment on the posterior tongue, and the presence of vesicular symptoms from the left side of the soft palate to the tonsillar pillar suggest glossopharyngeal nerve involvement.2 Although the involvement of glossopharyngeal nerve in herpes zoster is rare, it should be considered in the differential diagnosis of pharyngitis, particularly in the elderly and immunocompromised patients.3
Answer 2
VZV is an enveloped, double-stranded, linear DNA virus. The primary infection of VZV is transmitted either by aerosol or direct contact. It causes varicella (chickenpox) in children and pneumonia in adults. Exposure to VZV causes a cell-mediated immune response with production of immunoglobulin G, M and A.3 Immunoglobulin G (IgG) antibodies persist for life and provide lifetime immunity for varicella. The virus from the primary infection in the mucosa and epidermal cells spreads to the corresponding sensory nerves, where it remains dormant in the sensory dorsal root and cranial root ganglia. Reactivation of the virus results in replication and release of the virus in an entire dermatome. Increasing age1 or other factors contributing to decreased immunity3 lead to reactivation of the latent VZV infection acquired early in life and results in herpes zoster.
Answer 3
Acute VZV infection can be confirmed with polymerase chain reaction (PCR) assay obtained from vesicular lesions, cerebrospinal fluid and bronchoalveolar lavage. Direct immunofluorescence assay for VZV antigen, viral culture,4 and serologic testing for the presence of IgG antibodies are other tests employed to establish the diagnosis. It is important to test for herpes simplex and zoster to confirm VZV reactivation. Vesicular eruption may be absent in VZV-related cranial neuropathy, making viral identification essential to confirm the diagnosis.2 Although PCR is required for diagnostic confirmation, antiviral therapy is recommended within 72 hours of rash onset per Pharmaceutical Benefits Scheme recommendations and does not need to be preceded by viral confirmation.
Answer 4
Thoracic, lumbar, cervical and trigeminal dermatomes are typically involved in herpes zoster. Herpes zoster ophthalmicus and herpes zoster oticus are more common cranial nerve lesions in herpes zoster virus infection because of the involvement of ophthalmic division of the trigeminal (CN V) and facial (CN VII) nerves,5 respectively. Involvement of other cranial nerves is rare, but any autonomic ganglion or cranial nerve can be involved.2
Answer 5
Centor criteria6 identify patients who are likely to have a bacterial (streptococcal) cause of a sore throat and who are likely to benefit from antibiotics. Consider these criteria in patients with a sore throat before prescribing antibiotics.
Case continued
The PCR confirmed the diagnosis, and the patient was prescribed valacyclovir and pregabalin. The neuropathic pain worsened during the first week of treatment. It gradually began to improve after two weeks of treatment, and the patient’s condition improved significantly after four weeks.
Pain relief of herpes zoster is difficult because of its variety of presentations. The medication regimen is specialised for the individual patient and may require multiple drug combinations. Pregabalin dosing can be titrated up to target dose because of its linear pharmacokinetics, unlike gabapentin. Even though there is no proven efficacious benefit for pregabalin over gabapentin, this linear pharmacokinetic quality can be of benefit for adequate pain relief.7
| Table 1. Centor criteria from the National Institute for Health and Care Excellence guideline published in January 20186 |
| Centor criteria |
| Tonsillar exudate |
1 point for each finding |
| Tender anterior cervical lymphadenopathy |
| History of fever (>38°C) |
| Absent cough |
| Scoring recommendation |
| Score of 0, 1 or 2 |
Antibiotic therapy is not recommended |
| Score of 3 or 4 |
Consider an immediate antibiotic or backup antibiotic prescription |
Key points
- Increasing age or decreased immunity lead to reactivation of the latent varicella infection and results in herpes zoster.
- Consider herpes zoster involving the glossopharyngeal nerve in the differential diagnosis of pharyngitis, particularly in the elderly and immunocompromised patients.
- Consider Centor criteria before prescribing antibiotics in patients with a sore throat.