Case
A Caucasian female aged 15 years, with no significant medical history, presented to a regional acute care centre for assessment of a self-detected tender mass in her left breast. The mass had been present for three weeks, and the patient reported no nipple discharge, menstrual abnormalities or constitutional symptoms. On examination, there was an isolated 4 cm solid, mobile mass palpable in the upper inner quadrant of her left breast. There were no overlying skin changes, additional palpable breast masses or lymphadenopathy.
Question 1
What are the differential diagnoses for a breast lump in the adolescent female?
Question 2
What is the best approach to diagnosis?
Answer 1
The vast majority of breast masses in this population are benign yet may cause significant distress to the patient. Malignancy accounts for only 0.02% of surgically removed breast masses in the adolescent female.1 Fibroadenomas account for the majority of breast masses in this population, while other differentials include fibrocystic breast disease, fat necrosis, abscess, phyllodes tumour, intraductal papilloma and hamartoma. To date there have been only 13 cases of paediatric breast hamartomas reported in the literature.2–6 They invariably presented as a single painless palpable breast mass that had been present for 1–12 months prior to first presentation.
Answer 2
The ‘triple test’ approach provides a comprehensive algorithm for the investigation of a new breast symptom.7 This includes a detailed history and thorough clinical examination, followed by imaging and non-excisional biopsy. Ultrasonography is the preferred imaging modality for adolescents given the density of breast tissue in this age group. Fine needle aspiration cytology is appropriate for cystic lesions, while core biopsy is preferable for the investigation of suspicious lesions. Clinically, breast hamartomas are indistinguishable from the more common fibroadenomas or fibrocystic breast disease.6 However, the histological features are distinct, likely reflecting different origins. Histologically, they are characterised by densely packed enlarged lobules set within a fibrous stroma.8 The abnormal combination of normally occurring breast elements is thought to reflect a developmental malformation rather than a true neoplastic process.
Case continued
Ultrasonography showed an irregular hypoechoic mass at 11 o’clock, 4 cm from the nipple. The patient was referred to a breast surgeon for review, and a subsequent core biopsy revealed dense stromal fibrosis with no evidence of atypia or malignancy. A final diagnosis of breast hamartoma was made.
Question 3
What is known about the development of breast hamartomas in this patient population?
Question 4
Is there a risk of malignancy associated with paediatric breast hamartomas?
Answer 3
Breast hamartomas are uncommon benign lesions typically affecting women in their third or fourth decade of life.9 The likely role of female sex hormones in adolescent breast hamartoma development has been discussed elsewhere.4,8 Briefly, epithelial elements of hamartomas have been shown to express oestrogen and progesterone receptors in a pattern resembling normal breast tissue. The increased levels of oestrogen and progesterone during puberty may stimulate increased proliferation, thereby contributing to the development of hamartomas in adolescent females.8
Answer 4
There have been no reported cases of malignancy arising from breast hamartomas in the paediatric population. In the adult population, there have been few reported cases of recurrence or malignancy arising from breast hamartomas, and it is speculated that recurrent lesions may in fact represent multifocal disease rather than true recurrence.6,10
Overall there is a scarcity of literature documenting breast hamartomas in the paediatric population. Given the propensity for miscategorisation, the true incidence is likely to be higher than is currently indicated in the literature. Improved recognition and documentation of breast hamartomas in the paediatric population is necessary to improve our understanding of the incidence and natural history.
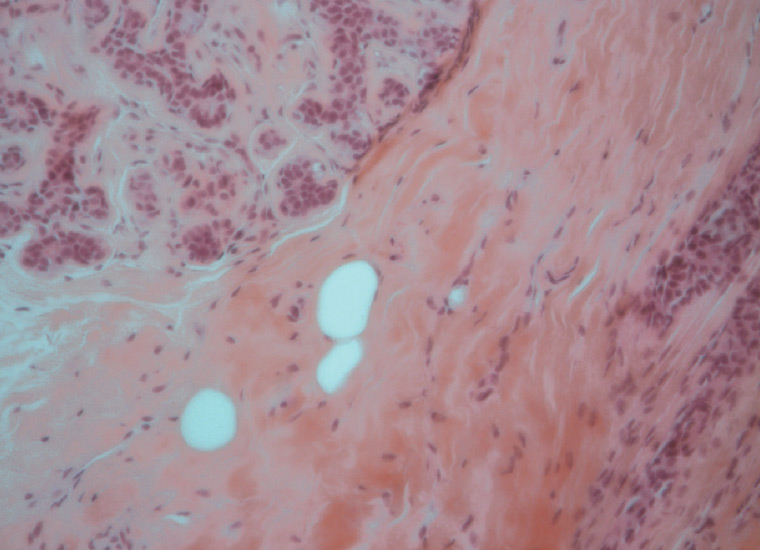
Figure 1. A histological sample of the biopsied lesion illustrating dense interlobular stroma
Case continued
The lesion remains in situ and will continue to be monitored by the breast surgeon on a six-monthly, then 12-monthly, basis given the likelihood of eventual involution.
Key points
- Breast hamartomas are rare benign lesions that are particularly uncommon in the paediatric population.
- Breast hamartomas are histologically distinct from the more common benign breast lesions.
- Adherence to a validated algorithm7 for investigation of a new breast symptom is crucial.
- There have been no reported cases of malignant changes in paediatric breast hamartomas.