Case
An uncircumcised man aged 70 years presented to a dermatology clinic with a three-month history of a persistent erythematous rash of the glans penis. He was initially managed with topical miconazole and doxycycline 100 mg daily for 28 days by his primary care physician with no marked improvement. The patient did not have any symptoms of pain, dysuria or pruritus. His medical history consisted of hypertension controlled with combination perindopril and amlodipine. There was no history of diabetes mellitus, cancer, sexually transmissible infections or skin conditions.
Question 1
What is the differential diagnosis?
Question 2
What examinations could help narrow the diagnosis?
Question 3
What initial investigations would be helpful?
Answer 1
The differential diagnosis for balanitis is summarised in Table 1.
| Table 1. Differential diagnosis for balanitis/balanoposthitis1–3,5,7–9 |
| Infective |
Inflammatory dermatoses |
Premalignant/malignant |
- Fungal (Candida spp.)
- Anaerobic (Bacteroides spp.,
Gardnerella vaginalis)
- Aerobic (Streptococcus spp.,
Staphylococcus spp.)
- Parasitic (Trichomonas spp., scabies)
- Spirochaetal (syphilitic and non-syphilitic)
- Viral (HSV, HPV)
|
- Zoon’s balanitis
- Psoriasis
- Circinate balanitis
- Eczema (allergic, irritant and seborrheic)
- Lichen sclerosus (balanitis xerotica obliterans)*
- Lichen planus
- Pemphigus vulgaris
- Fixed drug eruptions
|
- Squamous cell carcinoma in situ (Erythroplasia of Queyrat)
- Penile carcinoma (squamous cell carcinoma)
- Bowenoid papulosis
- Amelanotic melanoma
- Metastatic disease
- Kaposi’s sarcoma
- Extramammary Paget’s disease
- Basal cell carcinoma
|
*Lichen sclerosus is also considered premalignant
HPV, human papillomavirus; HSV, herpes simplex virus |
Answer 2
To narrow the diagnosis, it is important to perform a careful examination of genitalia and foreskin. This encompasses:1,2
- whether the penis is circumcised or uncircumcised
- skin lesion description
- size
- shape
- colour
- morphology
- distribution
- configuration
- secondary skin changes
- inflammation
- induration
- oedema
- discharge
- wounds (ulcers, erosion, chancres)
- atrophic changes
- hyperpigmentation/hypopigmentation
- hyperkeratosis
- inguinal lymphadenopathy
- other nodules or tumours
- other cutaneous or mucosal changes (eg nail pitting or gingivitis).
Dermoscopy may help differentiate common benign inflammatory conditions from premalignant/malignant causes. Common dermoscopic findings for several diagnoses include:3,4
- psoriatic balanitis – regularly distributed dots or glomerular vessels
- seborrheic/non-specific balanitis – irregular linear blurry vessels
- Zoon’s balanitis – focal/diffuse orange/yellow/brownish structureless areas +/– focused curved vessels (ie convoluted, serpentine or chalice-shaped) +/– dotted vessels +/– irregular linear lines
- squamous cell carcinoma in situ – scattered dotted vessels.
Answer 3
Helpful initial investigations include genital swabs with microscopy, culture and polymerase chain reaction testing for common infective causes such as:5
- Candida spp.
- herpes simplex virus
- human papillomavirus
- syphilis
- Trichomonas spp.
Case continued
On examination, there was a well-demarcated, eroded, erythematous patch involving the corona of the glans penis and inner prepuce surrounded by a white margin and multiple post-inflammatory hyperpigmented spots (Figure 1). There was no palpable inguinal lymphadenopathy or other skin or oral mucosal lesions noted on general examination. Genital swabs showed mix coliforms with no organism growth.
Benign inflammatory causes (Table 1) were suspected, and the patient was given hygiene advice and treated with topical corticosteroids for two months. On follow-up, the lesion had not fully resolved.
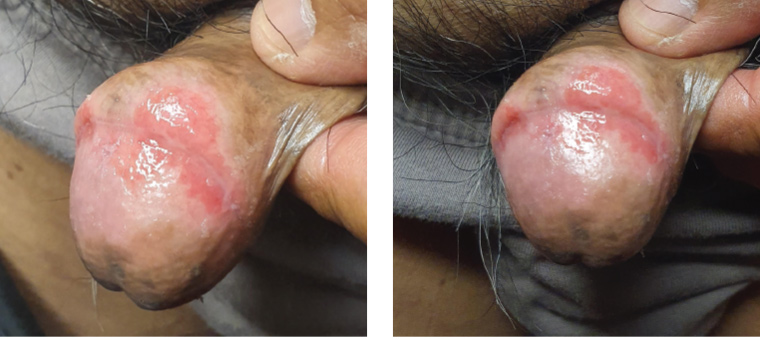
Figure 1. Lesion of the glans penis and prepuce
Question 4
What conditions must be ruled out in this patient, and how is this done?
Answer 4
Given the resistance to treatment with topical steroids, premalignant and malignant causes need to be ruled out via a punch biopsy for histopathological examination.
Other possible reasons for concern and biopsy include:1
- uncertain diagnosis
- no response to initial treatment after 4–6 weeks
- any erosive, hyperkeratotic or erythematous lesions
- new lesions (especially with lichen sclerosus or lichen planus).
Case continued
A 3 mm punch biopsy at the edge of the erythematous margin was taken. This showed focal lymphocytic infiltration, spongiosis and plasma cells; there was no evidence of malignancy.
Question 5
What is the likely diagnosis?
Question 6
How would this patient be managed?
Answer 5
The most likely diagnosis is Zoon’s balanitis, a benign disease occurring almost exclusively in uncircumcised older men and accounting for up to 10% of all reported balanitis cases.5,6 Its aetiology is thought to be associated with inadequate bathing and/or contextual ‘dysfunction’ of the prepuce, causing either urine retention, smegma build-up, friction or heat, which ultimately results in chronic irritation of the mucosa.5–7
It usually presents as shiny, moist, orange-red glazed, well-demarcated macule(s) with possible speckled orange-red plaques termed ‘cayenne pepper spots’.3,5
The diagnosis can be made clinically; however, a histopathological examination may be required to rule out malignancy and confirm Zoon’s balanitis.5 Common histological findings include epidermal thickening or atrophy with possible erosions and spongiosis, and infiltration of the dermal layer with predominantly plasma cells and hemosiderin deposits.3,5
Answer 6
Initial management of patients with balanitis/balanoposthitis without concerns for neoplasia includes general hygiene measures, topical antifungal medication and/or corticosteroids with regular follow-up (Table 2).
| Table 2. Specific management of Zoon’s balanitis3,5–7 |
| Management type |
Treatment options |
| General hygiene |
- Regularly retract foreskin, gently clean with warm water (avoiding soap) and thoroughly dry the entire glans penis, foreskin and prepuce
|
| Medical management |
- Topical corticosteroids +/– topical antibiotics
- Topical calcineurin inhibitors*
|
| Surgical management |
- Circumcision (definitive management)†
- Carbon dioxide laser therapy
|
*Topical calcineurin inhibitors have been shown to be effective; however, there is controversy regarding the risk of malignancy.
†Removal of prepuce will reduce irritants and friction. |
Zoon’s balanitis can be persistent and relapse even after general and medical management.7 Circumcision should be considered for patients with persistent symptoms who are non-adherent to general hygiene advice and/or refractory to medical management.6 Resolution post-circumcision is expected to occur between six weeks and several months.3
There is no current consensus regarding the follow-up timeframe for Zoon’s balanitis. Given concerns regarding malignancy (eg Erythroplasia of Queyrat), it is recommended to maintain regular follow-up for at least five years, with intervals dependent on the clinical progression and treatment used.3,5
Conclusion
Patients with balanitis commonly present to primary healthcare physicians. Given the concerns for more sinister causes such as malignancy, it is essential that general practitioners are confident in managing these patients.
Key points
- There is a variety of aetiologies for balanitis, including infective, inflammatory and neoplastic.
- Common infective and inflammatory causes may be empirically treated and followed up.
- Lesions that have not resolved despite treatment should be biopsied to rule out malignancy.
- Circumcision is an important management option for patients with balanitis