Case
A man aged 79 years who was living in a residential aged care facility and had an indwelling urinary catheter was noted by the caregiver to have ‘purple urine’ for more than a week (Figure 1). The patient had a medical history of transurethral resection of the prostate more than 10 years ago for benign prostatic hyperplasia and a history of laparotomy tumour resection with Hartmann’s procedure performed for sigmoid cancer four years ago. At presentation, he had no fever or symptoms suggestive of urinary tract infection (UTI). His bowel motion was normal. He was not taking any medication or herbal supplement. Physical examination was unremarkable. Urinalysis showed pH 8, nitrite (1+), protein (2+), blood (2+) and leukocytes (1+). A urine sample was collected for laboratory microscopy, culture and sensitivity analysis.
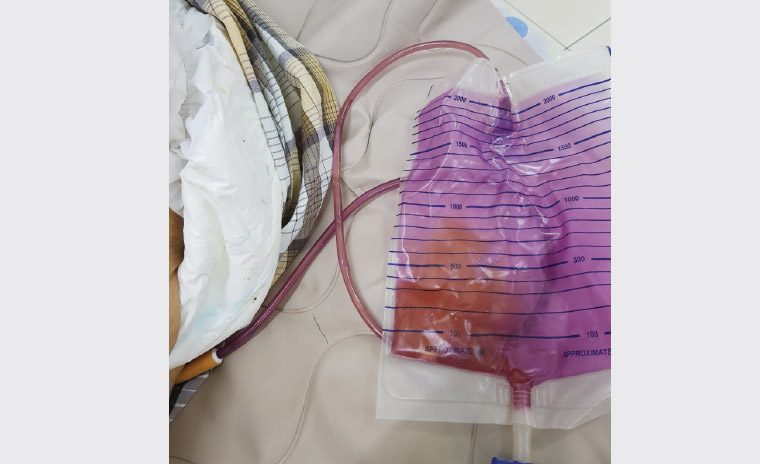
Figure 1. The yellowish urine is seen against the purple-stained urinary bag and tubing.
Question 1
What is the diagnosis?
Question 2
What is the pathogenesis for this phenomenon?
Question 3
What is the significance of this phenomenon?
Question 4
What is the differential diagnosis of purple urine bag syndrome (PUBS)?
Question 5
What are the risk factors for developing this condition?
Question 6
What would be the appropriate investigation?
Question 7
What is the treatment and how may it be prevented?
Answer 1
This patient likely has PUBS, as evidenced by the purplish staining of the urinary tubing and bag while the urine appears yellowish (Figure 1).
Answer 2
The purplish hue is the result of the interaction between the mixture of urinary pigments indirubin (red) and indigo (blue) with the urinary bag and tubing. These pigments are derived from the metabolism of tryptophan. Dietary tryptophan is metabolised by the intestinal bacteria into indoles, which are then absorbed into portal circulation. In the liver, indoles are converted into indoxyl sulphate and excreted in the urine. Bacterial sulphatases and phosphatases then act on indoxyl sulphate, producing indoxyl, which is oxidised into indirubin and indigo.1,2
Answer 3
PUBS is commonly associated with UTIs and constipation, although patients with this striking phenomenon often follow a benign course.2 However, it is important to note that there have been reports of critically ill patients with urosepsis who presented to emergency care with PUBS.3–5 In addition, PUBS has also been reported as the first sign of Fournier’s gangrene in immunocompromised patients and as an early indicator of multidrug resistant vulvar abscess and urinary drainage malfunction.2,6,7 Hence, when encountering any patient with PUBS, a thorough clinical history and physical examination is encouraged to ensure correct management.
Answer 4
Urinary discolouration can be caused by a range of conditions, including haematuria, myoglobinuria, lipiduria, porphyria, alkaptonuria and Pseudomonas spp. infection. Consumption of medicines including rifampicin, ibuprofen, phenytoin, propofol, L-dopa, flutamide, and certain foods such as blackberries, beetroots, carrots, fava beans and oral aloe therapy, among others, can also cause urinary discolouration.8,9 Notably for PUBS, the purple discolouration only involves the urinary tubing and bag but not the urine itself.1,8 In infants, this may represent Drummond syndrome, also known as ‘blue diaper syndrome’, in which excess indoles occur in urine due to abnormal tryptophan metabolism.8
Answer 5
Predisposing factors include:10
- advanced age
- female sex
- chronic urinary catheter use
- chronic constipation
- UTI, especially with high bacterial load
- alkaline urine
- aged care resident
- frailty or immobility
- dementia
- polyvinyl chloride urinary catheter
- chronic kidney disease/kidney failure
- dehydration.
Answer 6
There are no standard guidelines for the management of PUBS. As PUBS may be associated with an occult UTI with atypical symptoms, urinalysis and urinary culture is a reasonable first step.1,8 Further investigations will depend on signs of constitutional upset, such as fever or a change in conscious state (eg confusion). Extensive investigation is seldom needed.10
Answer 7
Mainstay treatments to be considered include antibiotic administration if a UTI is suspected, changing the urinary catheter and treating underlying constipation.5 Antibiotic use is recommended in symptomatic UTI, sepsis or immunocompromised patients.8 The need for empirical antibiotics in asymptomatic patients remains controversial and should be individualised.1,8 Prevention of PUBS involves managing the modifiable risk factors, which include regular review of the need for catheterisation; timely change of urinary catheter; good hygiene care with adequate hydration; and maintenance of normal bowel habit.1,8
Case continued
This patient had his catheter changed and he returned to the aged care facility. A week later, the ‘purple urine’ resolved while the urine culture showed mixed growth with significant colony count (>105 CFU/mL).
Key points
- PUBS, although mostly a benign phenomenon, may be associated with potentially sinister causes such as severe infection, sepsis and urinary drainage malfunction.
- Urinalysis and urine culture are needed if there is a suspicion of clinically significant urinary infection.
- Mainstay treatments include judicious use of antibiotics, changing of urinary catheter, treatment of constipation and good hygiene practices.