Up to 20% of children exhibit rapid jerky movements (motor tics) that are made without conscious intention as part of a developmental phase that often lasts a few weeks to months.1 Similarly, involuntary sounds, vocalisations or noises (vocal or phonic tics) such as coughing and even brief screams or shouts may be observed in some children for brief periods of time. Tics lasting for a few weeks to months are known as ‘transient tic disorder’. When single or multiple motor or vocal tics – but not a combination of both – have been present for more than one year, the term ‘chronic tic disorder’ is used. When both (multiple) motor and (one or more) vocal tics have been present for more than a year, with onset before the age of 18 years, the condition is known as Gilles de la Tourette syndrome (GTS) or, in short, Tourette syndrome.2
The aim of this article is to review current evidence regarding the assessment and management of GTS.
Prevalence
Once considered rare, GTS is now understood to be relatively common, occurring in approximately 1% of school-aged children.3 GTS is more common in boys, and the male-to-female ratio is estimated to be 4:1.4,5 Tics have a mean age of onset of 6–7 years, reach peak severity at the age of approximately 10–12 years, and typically improve by adolescence or thereafter.6
Clinical features
In addition to simple motor and vocal/phonic tics, complex tics may be present (Table 1). Some complex tics – such as spitting, licking, kissing, etc – may be misunderstood or misinterpreted and may result in the young person getting in trouble, especially if these tics include involuntary and inappropriate obscene gesturing (copropraxia) or copying the movements of other people (echopraxia). Similarly, complex vocal tics may include repeating words or phrases or even full sentences (echolalia) or repeating the last word or syllable (palilalia) or, in approximately 10–15% of cases, involuntary and inappropriate swearing or blurting out of obscenities (coprolalia).
| Table 1. Common tics of Tourette syndrome* |
| |
Simple
(involuntary meaningless movements) |
Complex
(unvoluntary seemingly purposeful movements) |
| Motor tic |
Eye blinking, eye rolling, squinting, facial grimaces, shoulder shrugging, arm extending, mouth opening, nose twitching, lip licking, head jerks, brushing or tossing hair out of eyes |
Pulling of clothes, touching people/objects, poking/jabbing, smelling fingers/objects, punching self, jumping/skipping, kicking, hopping, walking on toes, kissing self or others, feet shuffling, flapping arms, twisting around, twirling hair, self-injurious behaviour, biting, picking skin or scabs |
Vocal/phonic tic
|
Throat clearing, grunting, snorting, yelling/screaming, sniffing, barking, laughing, coughing, spitting, squeaking, humming, whistling, honking |
Making small animal-like sounds, unusual changes of pitch and volume of voice, stuttering, repetition of sounds
|
| *This is not an all-inclusive list |
Tics are usually preceded by a premonitory sensation or urge, such as a feeling of tightness, stretch, tension or itching that is relieved by performing the tic, thereby leading to an urge-tic-relief cycle.7,8 Patients with GTS may also exhibit a number of associated behaviours such as rage, self-injurious behaviours or non-obscene socially inappropriate behaviours that involve socially inappropriate comments or actions.9 Attention deficit hyperactivity disorder (ADHD) is encountered in approximately 60–75% of children with GTS, while obsessive-compulsive disorder (OCD) is reported in 27%, obsessive-compulsive behaviours (OCB) in 32%, and self-injurious behaviours in 25%.10 Although less common, features of autism, learning difficulties, anxiety, depression, phobia, irritability, impulsivity, rage, aggression, sleep difficulties, oppositional or conduct problems, substance use or personality issues may co-exist.11 Some individuals’ overall academic and social functioning as well as quality of life (QoL) may be affected more by these associated problems than the tics themselves.12 Regarding the age of onset, it is noteworthy that symptoms of ADHD may appear between three and six years of age (ie before the tics manifest), while the OCD symptoms usually manifest in late childhood or adolescence.
Tics can come and go, and they take a waxing and waning course. While tics are involuntary, they are sometimes referred to as ‘unvoluntary’ because the person may be able to suppress the tics for a period of time, and some of the complex tics may be camouflaged to look like purposeful movements. Thus children may voluntarily suppress their tics for short periods of time that may vary from seconds to minutes or hours, but this is at the expense of mounting inner tension and is often followed by a rebound or increase in tics. For example, some children may manage the school hours fairly well without many observable tics but then show increased frequency when they return home. This may lead to a misunderstanding that children can suppress the tics if they try harder. If anxiety and stress worsen the tics, then they may be mistaken as ‘psychological’ in origin. Rarely, tics may be brought on, or made worse, by a bacterial (eg group A streptococcus) infection such as in paediatric autoimmune neuropsychiatric disorder associated with streptococcal infection.
Aetiology
Genetics play a major factor in the development of GTS, but the mechanisms are complex. While no single susceptibility gene of large effect has been identified as yet, twin and family studies suggest that it is highly heritable, with a population-based heritability estimate of 0.771.13 Environmental factors are also involved, such as pre- and perinatal factors including difficulties with pregnancy, smoking, exposure to infection, immune or inflammatory factors and psychosocial stressors, as well as birth complications.14 Corticostriatal circuitry is implicated in GTS, with excess dopamine levels thought to be the underlying neurochemical abnormality.
Assessment
Assessment should include a detailed history inquiring about not only tics but also other associated conditions including ADHD, OCD and OCB, in the patient as well as among family members. Tics should be distinguished from involuntary movements due to other conditions (Table 2).5 Careful neurological examination may provide reassurance for the patient, parent/carer and doctor.
Once a diagnosis is made, further assessments should include those of comorbid conditions, associated features and the impact of their symptoms (Figure 1).
| Table 2. Differential diagnosis of Tourette syndrome5 |
| Diagnosis |
Characteristic feature |
| Gilles de la Tourette syndrome |
Onset at approximately 6–7 years of age, with further emergence of symptoms that peak at approximately 10–12 years of age, and remission post-adolescence; waxing and waning course; the type and site of tics changes from one place to another; voluntarily suppressible for short periods of time |
| Athetoid type of cerebral palsy |
Onset between birth and three years of age; static course; associated neurological deficit and learning disability |
| Dystonia musculorum deformans |
Torsion dystonia of legs – progressive; crippling 10–15 years after onset |
| Spasmodic torticollis |
Associated with spastic speech; static or progressive |
| Encephalitis lethargica |
History of encephalitis, Parkinsonian symptoms |
| Huntington’s chorea |
Onset in third to fifth decades (1% in early childhood); usually a positive family history of Huntington’s chorea; choreoathetoid movements; dementia; progression to death in 10–20 years |
| Other involuntary movements |
Myoclonus: shock-like, arrhythmic twitches; not suppressible
Chorea: dance-like, unpatterned movements; often approximate a purpose (eg adjusting clothes, checking a watch); often rapid, involving proximal or distal muscle groups
Athetosis: writhing movement, mostly arms/hands; often slow
Dystonia: sustained or repetitious muscular contractions; often produces abnormal posture
Hemiballismus: wild, large amplitude, flinging movements on one side of the body, commonly affecting proximal limb muscles but can also affect the trunk |
| Tardive tourettism |
History of long-term use of neuroleptics, levodopa or other medications |
| Other neurological disorders |
Signs and symptoms specific to the disorder such as autistic disorder, post-stroke, Sydenham’s chorea, multiple sclerosis, Wilson’s disease, Hallervorden-Spatz disease, Jakob–Creutzfeldt disease, choreoathetosis, neurofibromatosis, Arnold–Chiari malformation and status dysmyelinatus |
| Acquired tourettism |
Onset in adulthood; trauma; carbon monoxide poisoning; basal ganglia infarct |
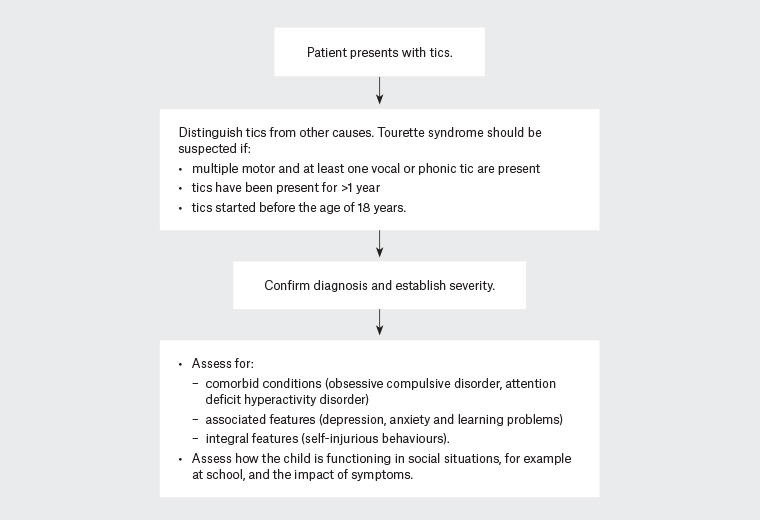
Figure 1. Assessment of patients presenting with tics
Social impact and quality of life
Tics can affect a child’s life in a number of ways; these include the impact on school and academic work, social life and relationships as well as physical and mental wellbeing.12 The visible nature of the tics may draw attention to the individual or lead to embarrassment, teasing/bullying or social exclusion.
Impact on school work may be due to the effect of tics on learning or due to related conditions such as ADHD, OCD/OCB or an associated learning disorder.15 The ability to focus in class and engage in school activities may be reduced as a result of the child spending time and energy on trying to hide or suppress the tics while at school. Other students or teachers may accuse the individual with tics of deliberately ‘pulling faces’, spitting or disturbing the class through grunts or vocalisations.
QoL has been shown to be lower in people living with GTS when compared with the general population.16 Among patients with GTS, individuals without comorbidities have been found to have better QoL than those with comorbidities.17 Parent-reported comorbidity in children and adolescents with GTS has been found to be associated with decreased QOL, increased emotional symptomatology and impaired emotional, social (including peer relationship) and school functioning.18 Warm and supportive family relationships are integral to long-term social and emotional stability in children with GTS and their QoL.12
Management
Management options for children and young people with GTS include education, explanation and advice; linking with support groups; and behavioural interventions as well as medication. A decision tree on management is outlined in Figure 2.2
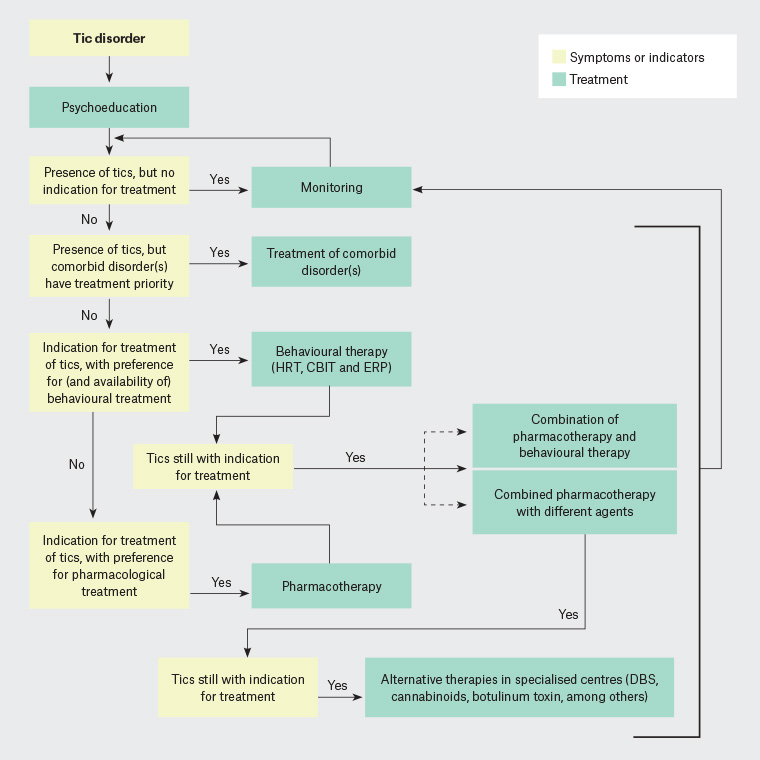
Figure 2. Decision tree for the management of Tourette syndrome
CBIT, comprehensive behavioural intervention for tics; DBS, deep-brain stimulation; ERP, exposure and response prevention; HRT, habit reversal therapy
Reproduced with permission from Robertson MM, Eapen V, Singer HS, et al, Gilles de la Tourette syndrome, Nat Rev Dis Primers 2017;3:16097, doi: 10.1038/nrdp.2016.97.
It is noteworthy that only approximately 10% of patients with GTS have ‘pure Tourette’, where they present with only motor and vocal tics. Most patients with GTS have ‘Tourette-plus’, where one or more comorbid conditions are present (Figure 3).9 Management in these situations should take into account the symptoms that are causing most distress or dysfunction.
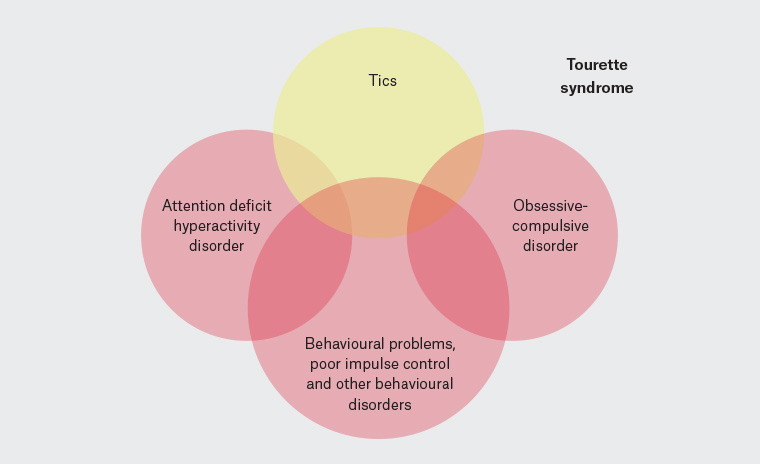
Figure 3. Conditions associated with Tourette syndrome
Education, explanation and advice
All affected children and their families need information about the nature and course of GTS and any accompanying conditions, and advice on how to manage tics. For mild cases, advice regarding tic management may be all that is needed. It is important to emphasise to the parents/carers and child that the tics are involuntary and outside the child’s control, and that they cannot help these sudden movements or voices/noises. A parallel may be drawn with trying to supress a sneeze or avoid blinking.
The young person and their family may be linked up with the Tourette Syndrome Association of Australia, and the health professional that they have consulted may provide information to schools or other environments in which the child interacts. The biological nature of tics should be highlighted, and it should be emphasised that they are not due to stress or ‘bad parenting’.
Following assessment and explanation about the nature of the condition, moderate cases may benefit from referral to a psychologist for behavioural methods of treatment. When the tics are severe with associated distress and/or dysfunction, or when significant comorbidities are present, the general practitioner (GP) may refer the patient to a specialist with expertise in GTS for a comprehensive assessment and management plan. GPs can refer to clinical psychologists under a mental healthcare plan for the implementation of behavioural treatments.
Behavioural methods of treatment
For children with mild-to-moderate tics, effective treatments include specific behavioural techniques such as exposure and response prevention (ERP), habit reversal therapy (HRT)19 and comprehensive behavioural intervention for tics (CBIT).20 In ERP, the patient is trained to stay exposed, endure the premonitory urge and prevent or resist performing the tic symptoms. In HRT, patients are trained to do competing responses instead of performing the tics, and the program consists of awareness training with self-monitoring, relaxation training and competing response training. CBIT combines awareness training with competing response training and social support. Following awareness training, patients are taught to engage in a ‘competing response’ every time the urge or tic occurs. The social support component involves teaching the patient’s parent (or another person) to praise the patient for using the competing response correctly and to remind the patient to use the competing response.
Medication
For moderate-to-severe tics and other features of GTS causing either distress or dysfunction, it is worthwhile considering medication. The following medications may be useful.
Centrally acting α-adrenergic agents such as clonidine or guanfacine are usually the first line of treatment, especially if tics and hyperactivity are both present. It is important to monitor blood pressure as these agents can cause hypotension. There is also a risk of rebound hypertension if the medication is ceased abruptly.
Small doses of antipsychotics, such as risperidone, aripiprazole, amisulpride or haloperidol, can help control the tics. It is recommended that patients are prescribed a low dose, which is then increased slowly if side effects do not occur. First-generation antipsychotics such as haloperidol have been the treatment of choice since the 1960s but are used less frequently nowadays because of the risk of extrapyramidal syndromes. Weight gain and metabolic effects need to be monitored when a patient is prescribed second-generation antipsychotics such as risperidone or aripiprazole. When considering the choice of medication for tics, the effects of the medication on comorbid disorders also deserve consideration. For example, clonidine can be useful when the patient also has ADHD and sleep problems, while risperidone can have additional benefits when comorbid aggression and behavioural problems are present. Aripiprazole has been found to augment the therapeutic response to selective serotonin reuptake inhibitors in patients who also have OCD, anxiety or major depressive disorder.21
Less commonly used treatments that are typically reserved for complex cases with comorbid epilepsy and other complexities include anticonvulsants (eg topiramate, carbamazepine, levetiracetam), benzodiazepines (eg clonazepam) and cannabinoids.2
Although not used in children, in adults with severe refractory and treatment-resistant GTS, deep-brain stimulation (DBS) has been used with some success.22 DBS involves the implantation of electrodes for chronic stimulation aimed at modulating neuronal activity in target regions. There is significant heterogeneity in outcomes, and there is also a lack of consensus regarding the ideal brain target; therefore, further research is needed.
Conclusion
Tics are frequently under-recognised or misdiagnosed; simple tics may be discounted as habits, and complex tics as behavioural disorders. Increased awareness of the condition and better supports are sorely needed.
Key points
- Motor tics occur in up to 20% of children as a developmental phase but usually do not last longer than a year.
- GTS is diagnosed when there are several motor tics and at least one vocal tic that have been present for more than a year.
- GTS occurs in around 1% of school-aged children.
- Tics usually appear around the age of 6–7 years, increasing in severity until the age of approximately 10–12 years, after which they start to reduce and – in the majority of cases – become considerably better by young adulthood.
- For mild cases, explanation and advice about the condition may be sufficient, while moderate-to-severe cases will benefit from referral to a specialist with expertise in the assessment and management of GTS.
- No single cause has been found for GTS, but the major contributing factors include genetics and pre- and perinatal difficulties.
- Ninety per cent of people living with GTS will experience comorbid conditions such as ADHD or OCD/OCB or associated features such as depression and anxiety.