Various topical corticosteroid (TCS) agents and potencies are available for the treatment of dermatological disorders such as atopic dermatitis, contact dermatitis, psoriasis and lichenoid disorders in patients of all ages. However, studies have shown the existence of steroid phobia among non-dermatologist professionals (eg general practitioners [GPs] and pharmacists) as well as patients and parents, evidence of non-adherence and unresolved outcomes of skin conditions affecting quality of life and healthcare costs.1–8 Therefore, selection of TCS agents for effective treatment without undesirable effects is essential.
How simple is it, and what do we need to know to select the correct TCS for effective treatment of a particular condition? TCS agents have different formulations, percentages and molecular structures despite similar or near-similar names. These variations affect the potency, efficacy and effect. In addition, there are variable classification systems for the potency of TCS agents.9–12 Therefore, it is important to determine the potency of the TCS correctly for treatment. This article highlights the various potency categories of TCS agents for effective treatment of dermatoses from the general practice perspective.
Topical steroid selection and potency categories
The potency of TCS agents has been historically measured by the intensity of the vasoconstrictive effect.13 However, the specific molecular structure (eg betamethasone valerate or dipropionate), formulation (cream, ointment or solution) and percentage (eg 0.05% or 0.1%) all affect the potency. In addition, the skin application site, use of an occlusive dressing and the vehicle (base) may alter or enhance the effect of the steroid, in accordance with the following general principles:
- Ointments penetrate skin slightly better than creams.
- Areas with thin skin (eg the face and eyelid) absorb medicine more readily than areas with thick skin (eg the trunk, limb, hand and foot).
- Intertriginous areas (eg the axilla, groin and breast folds) retain topical medications longer, with increased absorption.10,14
Thus, it is imperative to consider these factors along with the potency of the TCS for effective selection.
Regarding the classification of TCS potency, in 1997 the World Health Organization introduced class I (ultrahigh, the most potent) to VII (low, the least potent).9 However, some countries established a reversed order as well as use of several subdivisions with ill-defined words (eg low, weak, mild and medium in potency), leading to confusion for practitioners in complicated cases. Australasian guidelines favour the categories of mild, moderate, potent and very potent with corresponding classes I to IV, as shown in Table 1.1,3,12
| Table 1. Classification of topical corticosteroid (TCS) potency in Australasia1,3,12 |
| Potency |
Corticosteroid |
Mild
[Class I] |
- Hydrocortisone 0.5–1%
- Hydrocortisone acetate 0.5–1%
|
Moderate (mid-strength)
[Class II] |
- Clobetasone butyrate 0.05%*
- Hydrocortisone butyrate 0.1%*
- Betamethasone valerate 0.02–0.05%
- Triamcinolone acetonide 0.02–0.05%
- Methylprednisolone aceponate 0.1%†
|
Potent
[Class III] |
- Betamethasone dipropionate 0.05%
- Betamethasone valerate 0.05–0.1%
- Mometasone furoate 0.1%
|
Very potent
(ultra/super-potent)
[Class IV] |
- Clobetasol propionate 0.05%
- Betamethasone dipropionate 0.05% in optimised vehicle
|
Note: TCS agents unavailable in Australia are not listed here.
*Not available under the Pharmaceutical Benefit Scheme subsidy
†Placed in the potent group by some countries |
Overall, the choice of potency will largely be guided by the following factors:
- patient: age (infant, child or adult) and lesion location
- lesion: type and severity of lesion (as described in Table 2)
- topical medication: molecular structure, percentage and formulation/vehicle
- method of application: occlusive dressing increases potency with better efficacy and effect, and wet dressing intensifies the effect by improved permeability of topical medication.
Table 2 lists multiple skin conditions treatable with TCS agents.15–17
| Table 2. Common skin conditions treatable with topical corticosteroid (TCS) agents15–17 |
Mild (low) potency TCS
|
- Dermatitis (face, eyelids, napkin area)
- Intertrigo
- Perianal inflammation
|
Mild-to-moderate potency TCS
|
- Atopic dermatitis
- Asteatotic eczema
- Contact dermatitis
- Dry nummular eczema
- Perianal inflammation (severe)
- Intertrigo (short term)
- Scabies (after scabicide)
- Seborrhoeic dermatitis
|
Moderate-to-potent/ultrapotent TCS
|
- Atopic dermatitis (severe)
- Alopecia areata
- Contact dermatitis (severe)
- Eczema of hyperkeratotic, exudative nummular, hand and feet
- Granulomatous skin disorders – Granuloma annulare, Necrobiosis lipoidica, and sarcoidosis
- Lupus erythematosus
- Lichen – simplex chronicus, planus and sclerosus
- Pemphigus and pemphigoid
- Psoriasis
- Stasis dermatitis
- Vitiligo
|
| Note: Interchangeable choice of TCS with titration and response can be applied in some conditions as per description by factoring or specific local guidelines. Some hypertrophic/hyperkeratotic lesions might also require a combined intralesional steroid injection, which is beyond the scope of this article. |
Topical corticosteroid application
With regard to choice of TCS formulation, an ointment base is preferred for dry, scaly and mucocutaneous lesions (eg on the lips and genitals); cream for wet/oozing lesions; and liquid (solution, lotion) for hairy areas (eg scalp), where cream or ointment is unable to reach the areas of affected skin.
The advice of applying TCS agents ‘sparsely’ is no longer applicable; instead, ‘liberally’ is encouraged. The required dose (amount) is guided by location and extent of the lesion (Box 1). The fingertip unit (FTU) is a useful general guide for the amount of topical agent (Figure 1).1,3,14,18
| Box 1. Dosage calculation of topical corticosteroids (examples guide; 1 FTU = 0.5 g) |
- A child aged six years with face and neck involvement requires 2 FTU (1 g) daily, and a 15 g tube of topical corticosteroid (TCS) would last two weeks.
- An adult with one leg and foot involvement requires 8 FTU (4 g) daily, and two tubes of 15 g TCS or one tube of 30 g would last one week.
- Greater quantities of the 15 g tube of potent TCS can be prescribed under the Pharmaceutical Benefits Scheme streamlined authority with the repeat, depending on the percentage of body surface involvement, which is to be calculated from rule of nines (similarly for burns).
|
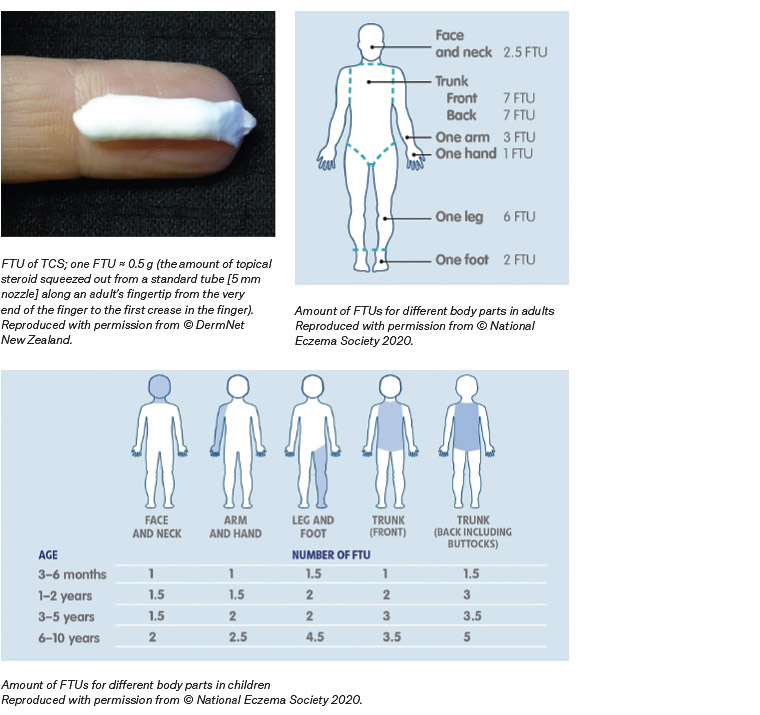
Figure 1. Fingertip units (FTUs) of topical corticosteroid (TCS) per application1,3,14,18
It is highly recommended to use adjunct moisturisers/emollients following application of TCS agents to affected areas. The moisturiser can be applied locally or to the whole body to ease pruritus and irritation by maintaining optimum skin moisture. The moisture alone is also useful as a steroid-sparing agent in trivial dermatitis. Diluting the topical steroid with moisturiser does not change the potency of the medicine.12,14 Application is usually encouraged in the evening/night after bathing to avoid incidental removal of the medication as a result of day-to-day activities. In terms of frequency, a once-daily regimen is generally recommended for better compliance. Twice-daily application may be considered for the initial week(s) for certain severe lesions, reducing to daily or alternate-day application depending on the response.
An occlusive dressing with appropriate cover, such as a tubular bandage or plastic wrap, is favourable for severe and thick/keratotic/lichenified lesions. Occlusion with a non-irritant glove or sock can also be used for lesions of the hand or foot, respectively. Close monitoring of occlusive or wet dressings is important to avoid undesirable effects from the reaction of occlusive materials and systemic absorption.
The duration of treatment depends on the type and intensity of the lesion; it is also guided by response to treatment, or follows a specific local guideline if available. It is advisable to discontinue or phase out application from daily to alternate-day, twice-weekly or weekend use over weeks or months (depending on the nature of residual lesion and recurrence) once the active inflammation/lesion has subsided. However, continued application of moisture should be encouraged.
Adverse effects
Topical steroids work via their anti-inflammatory, immunosuppressive and antiproliferative effects. Adverse effects, such as skin atrophy, striae, telangiectasia, easy bruising and hypertrichosis, are rare if TCS agents are used correctly.1,3,14 Periorificial dermatitis, steroid rosacea, red skin syndrome, contact dermatitis and pigment alteration are uncommon, and hypothalamic–pituitary–adrenal axis suppression is extremely rare. Nevertheless, it is necessary to be mindful of iatrogenic Cushing’s syndrome, growth retardation, cataract and glaucoma due to systemic absorption; such occurrence might be attributed to prolonged misuse of potent or ultrapotent TCS agents over large skin areas and/or occlusion causing increased systemic absorption, especially in susceptible individuals (young children and elderly patients with thin skin).14,19,20 In fact, adverse effects are more frequently reported in countries where higher-potency TCS agents are easily available over the counter or with the misuse of steroid in unregulated products.14,19,21 Adverse effects of TCS agents are generally reversible by cessation of medication. Emerging evidence suggests that methylprednisolone aceponate and mometasone furoate are associated with lesser local and systemic adverse effects than older formulations of TCS because of their lipophilic structure and pharmacokinetics.22–25 Mild-to-moderate-potency steroids and short-term use of potent topical steroids are safe in pregnancy and lactation according to a systematic review (Chi et al).14,26
Overall, the benefits significantly outweigh any unwanted effects if TCS agents are correctly prescribed. Undertreated conditions are more widespread than overtreatment.1,3,12,14 Therefore, it is prudent for practitioners to properly educate the users to avoid non-adherence from steroid phobia, and undertreated conditions.
Case examples with choice of topical corticosteroid
Case 1
A girl aged five years presented with dry atopic dermatitis of both hands. The dorsum hand location, which had some degree of scaling, was considered in selection of a TCS of moderate potency – methylprednisolone aceponate 0.1% ointment. One FTU to each hand with additional moisturiser cream nightly under non-irritant cotton gloves was applied. Total improvement was achieved in two weeks, and the patient’s mother was advised to continue twice daily application of moisturiser to the patient’s hands.
Case 2
A young man aged 20 years presented with lichen simplex chronicus (thick, scaly and cracked skin) on the dorsum of the right foot, which had failed to respond to intermittent use of a mid-strength TCS. Treatment consisted of two FTUs of potent TCS (betamethasone dipropionate 0.05% cream) twice daily with an occlusive wet dressing (tubular bandage) for one week, followed by continuation of the potent TCS daily with occlusion at night after review. A satisfactory outcome was achieved in four weeks, and the patient was advised to continue the TCS twice weekly for a further eight weeks with the application of daily moisturiser to minimise recurrence. The patient was encouraged to apply daily sunscreen or moisturiser, and reassured that the skin, which displayed post-inflammatory hyperpigmentation, would return to normal colour in 3–6 months.
Case 3
A man aged 55 years with penile lichen sclerosus presented with complications of fissures, pain and phimosis following failed treatment with mild-potency topical hydrocortisone 1% cream, prescribed by another institution one year ago. While waiting to be seen by a urologist for circumcision, he was treated with a potent TCS (mometasone furoate 0.1% ointment, 0.5–1 FTU) twice daily for one week, and then daily after review. At six weeks, the skin had become normal in texture with no fissures, and the foreskin was able to be partially retracted.
In short, each case should be able to be treated effectively by factoring in patient and lesion characteristics, potency of TCS and method of application, as described in the ‘Topical steroid selection’ section. Complex or recalcitrant cases require referral to a dermatologist.
Conclusion
Ensuring the right potency of TCS by taking into consideration the relevant factors is important to avoid undertreating conditions of steroid-responsive dermatological disorders in clinical practice. It is apparent that the benefits from appropriate use of TCS appreciably outweigh the uncommon adverse effects.
Key points
- Careful selection of TCS potency by taking into account implicated factors is crucial for successful treatment of steroid-responsive skin conditions.
- It is prudent for GPs to effectively educate the users to avoid non-adherence from steroid phobia and undertreated conditions.
- TCS agents approved for a variety of dermatological disorders are safe and effective if correctly applied, and are also inexpensive