Benefits of regular physical activity on physical and emotional health are well documented and widely accepted.1 Short-term benefits include improved mood, promotion of weight loss and maintenance of cardiovascular fitness. Longer-term benefits for both mother and child include weight management, reduction in chronic cardiometabolic disease, management of mental health and modelling healthy behaviours for families. There is strong evidence that exercise is beneficial for the majority of Australia’s national health priorities.2
Exercise during pregnancy is strongly recommended3 and can be performed safely without risk to the mother or fetus.4 Women who remain active during pregnancy are more easily able to incorporate an exercise routine postpartum.
Despite these benefits, many women do not return to pre-pregnancy physical activity levels, with a sharp decline in physical activity levels reported three years postpartum.5 Common barriers include physical discomfort, social isolation, financial constraints and difficulties in prioritising health over competing responsibilities.
General practitioners (GPs) have the potential to contribute to far-reaching societal implications by helping women return to physical activity after giving birth. The most common specific barriers, as detailed in this article, relate to musculoskeletal structures (in general) and specific pelvic trauma related to childbirth (whether by Caesarean section or vaginal delivery). A suggested list of referrals and indications is included in Box 1.
| Box 1. Suggested referrals and indications |
- Sport and Exercise Physician – Exercise prescription and return to activity/management of RED-S/diagnosis of musculoskeletal injuries
- Pelvic health physiotherapist – Assessment, diagnosis, education, equipment prescription and exercise programs, including pelvic floor muscle training
- Musculoskeletal physiotherapist – Management of musculoskeletal injuries
- Podiatrist – Management of foot pain postpartum, footwear advice
- Dietitian – Management of nutritional needs/assistance with weight loss/management of RED-S
- Psychologist – Behaviour change in the management of weight gain/RED-S/management of postnatal depression
- Continence nurse – Assistance with the management of faecal and bladder incontinence
- Lactation consultant – Assistance and education if breastfeeding difficulties arise
- Exercise physiologist – Individualised exercise prescription and safe return to the gym
- Urogynaecologist – Management of a grade 3–4 pelvic organ prolapse
- Colorectal surgeon – Management in the event of a third- or fourth-degree tear
|
| RED-S, relative energy deficiency in sport |
Challenges to return to exercise faced by women in the postpartum period
Musculoskeletal issues
Lower back and pelvic girdle pain
Up to 50% of women experience pregnancy-related pelvic girdle pain (PGP) or lower back pain during pregnancy and in the postpartum period. Although most recover spontaneously soon after delivery, up to 20% report pain persisting for years.6 Caesarean delivery increases the risk of severe persistent PGP six months postpartum.7
Early intervention with exercises focusing on dynamic control, ergonomic advice and development of strength and endurance is recommended as first-line management.8
Hand and wrist problems
De Quervain’s tenosynovitis (inflammation of the tendon sheath of the first extensor compartment of the wrist) is commonly seen in the postpartum period. This occurs as a consequence of new and repetitive movements (ie lifting, holding and nursing a newborn).9 In other contexts, it is managed by reducing wrist and hand loading, but this can be very difficult for a new mother until a time when the child can walk independently. For this reason, it is best managed using a thumb immobilising splint. A corticosteroid injection is an option for reducing symptoms in severe cases; however, this can affect breastmilk supply so requires careful consideration.10 Not enough attention is given to prevention, which would be to regularly use the wrist for similar tasks pre-birth so that the upgrade in load from lifting is not as sudden.
Diastasis recti abdominis
The rectus abdominus is the most superficial of the four abdominal muscles and consists of two separate muscle bellies enclosed by a fascial layer, joining at the midline to crease the linea alba. Diastasis recti abdominis (DRA) occurs as a result of stretching of the linea alba during pregnancy, separating the muscle bellies of the rectus abdominus. This expansion is a natural adaptation during the later stages of pregnancy and childbirth, although many women experience longer-lasting dysfunction, with an incidence of 60% at six weeks and 32.6% at 12 months postpartum.11
Specialist referral and exercise prescription by a qualified women’s health physiotherapist is recommended with a graduated return to abdominal strength, function and control. Patients with DRA need a cautious and gradual approach to reloading and often have challenges with abdominal-dominant exercise programs in the early postpartum period. There has been some controversy surrounding surgical repair of DRA after pregnancy. In 2016 it was removed from the Medicare Benefits Schedule (MBS) because of concerns that funding was being used for cosmetic purposes; however, it is expected to return to the MBS in 2022. Surgery is not the first line of treatment for DRA postpartum12 but may be considered in cases where DRA limits function and decreases quality of life.
Pelvic floor and related issues
Physiological changes to a woman’s body during pregnancy and the consequential strain on her pelvic floor begins long before the onset of labour. Risk factors for pelvic floor injury include multiparity and vaginal delivery; however, pregnancy alone is a risk factor for pelvic floor dysfunction.13
After childbirth, approximately one in three women experiences urinary incontinence, and up to one in 10 has faecal incontinence. Up to half of all women who have had a baby will have some degree of pelvic organ prolapse.14 Incontinence and prolapse can decrease quality of life, are risk factors for anxiety and depression and are significant barriers for returning to exercise after giving birth.15
In the postnatal period, women can benefit from individualised assessment and guided pelvic floor rehabilitation for prevention and management of urinary incontinence and pelvic organ prolapse, and improved sexual function.16 Consequently, educating women in the postnatal period about optimal health choices, including correct pelvic floor muscle training as part of safe return-to-exercise guidance, is a priority for primary care (Box 2).
| Box 2. Pelvic floor functions and symptoms that may warrant referral |
Five functions of the pelvic floor
- Maintain urinary and faecal continence
- Support pelvic organs (bladder, bowel and uterus)
- Provide support during pregnancy and aid vaginal childbirth
- Assist in sexual function
- Work as part of the ‘core’ muscle group to maintain stability and generate intra-abdominal pressure.
Pelvic floor signs and symptoms that may warrant a referral
- Accidental leakage of urine with a cough, sneeze, laugh, lifting, exercise
- Inability to hold onto urine on the way to the toilet
- Sudden urgency to urinate or defecate
- Inability to hold onto wind
- Painful intercourse
- Needing to strain on the toilet, with or without pain
- Feeling of heaviness or dragging in the vagina
- Not recognising the urge to urinate
|
Weight management and relative energy deficiency in sport
Weight gain
On average, weight retention one year postpartum ranges from 0.5 kg to 4 kg.17 Excessive weight retention postpartum is associated with increased long-term risk of obesity, type 2 diabetes and cardiovascular disease.18
Increased energy intake and nutritional choices, together with a decrease in exercise levels (energy expenditure), is the main contributing factor to weight gain. A perceived lack of time for meal preparation and exercise needs to be addressed holistically.
Relative energy deficiency in sport
Relative energy deficiency in sport (RED-S) refers to a situation in which a person does not take in enough energy to fuel the demands of exercise and daily living. It can affect many aspects of physiological function including menstrual function, bone health and psychological health.19 The lifestyle of a new mother is often coupled with sleep deprivation, change in nutritional habits, lack of routine and increased nutritional demands of breastfeeding (estimated to be approximately 600 kcal/day), predisposing to RED-S and the sequelae. It is important to ask about these on history and consider bone stress injuries in the new mother who presents with musculoskeletal pain on returning to exercise.
Mental health: Postnatal depression
Postnatal depression (PND), defined as depression occurring within 12 months after giving birth, is experienced by approximately 20% of women.20 However, up to 50% of women experience high levels of depressive symptoms without a formal diagnosis of PND. Exercise is a well-recognised treatment modality for depressive symptoms; in certain instances, it is as effective as pharmacological treatments.21 It has been shown to improve emotional wellbeing and reduce symptoms of anxiety and depression in the postpartum period.3
Exercise prescription postpartum
A return-to-exercise program postpartum needs the same level of consideration, graduation and rehabilitation that is required after ligament, tendon, muscle or bone injury. GPs are increasingly prescribing exercise, although the skills to do so have not traditionally been part of medical school teaching and training.22 Tissue recovery can take 4–6 months postpartum, well beyond the traditional six-week postpartum review. Caution needs to be taken to ensure an individualised and gradual return-to-exercise program (Figure 1) with consideration given to medical history, exercise history and complications during pregnancy and birth.
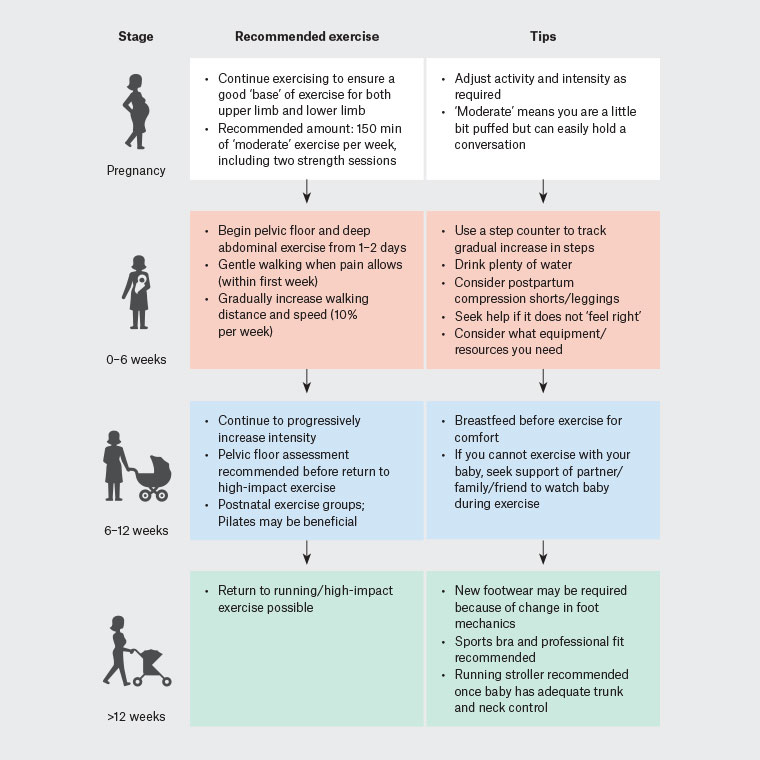
Figure 1. Return to exercise post pregnancy
Almost one-third of Australian mothers give birth via Caesarean section.23 Mothers who have birthed their babies via Caesarean section or operative vaginal delivery (episiotomy, use of forceps, potentially vacuum) will have slightly longer recovery timeframes, compared with those with uncomplicated vaginal deliveries.24 Consequently, this will affect their return-to-exercise plan, and a healthcare professional should be consulted before returning to any form of exercise before six weeks postpartum. During the first week following a Caesarean section, activities in the home (or hospital stay) should be limited to personal care and care for the baby only. By the third week, home activities may be resumed, and specific care of the incision site should be taken, including limiting stretching, until the wound is healed, which is expected at six weeks postpartum.25 Gentle exercise, such as deep breathing and walking, can actually be effective in reducing pain following Caesarean section.26
Exercise prescription during pregnancy is strongly recommended and requires consultation with the patient’s GP or obstetrician to ensure safety for the mother and fetus. Women who remain active during pregnancy are more easily able to incorporate an exercise routine postpartum.
Case studies
Case 1
A female patient aged 29 years presented to her GP asking for advice about a return to running after an uncomplicated vaginal delivery from her first pregnancy. Prior to her pregnancy, she was competing in 5 km parkrun events and training towards a marathon. She was able to keep running until the start of the third trimester. Her pre-pregnancy weight was 56 kg, and her weight was 74 kg immediately after birth. Her main question was when it was ‘safe’ to start running. Her GP advised that guidelines suggest three months, although it depends on pelvic floor status. Amateur athletes tend to return to exercise less quickly than those at the elite level.27 The key is to start gentle walking a few days after hospital discharge and to gradually increase the amount and intensity of walking. She was advised that trying to ‘bridge’ from walking to running is safest (ie progressing from challenging walking, including hills and at a brisk pace, to very easy running), which she managed to do at week 10 after giving birth. She was advised not to be competitive in her running for at least 4–5 months. At six months postpartum, the patient was able to finish a 5 km parkrun event in 24 minutes. Her weight was 59 kg, and she was thrilled to be able to enter an event.
Case 2
A female patient aged 34 years presented to her GP wanting advice about whether she needed to start exercising after giving birth by Caesarean section. The patient was, in her own words, ‘not a great exerciser prior to pregnancy’. Her pre-pregnancy weight was 68 kg. She weighed 94 kg after giving birth, and she developed gestational diabetes during the pregnancy. She was advised that regular light-to-moderate exercise was vital for general health and that postpartum was as good a time as any to make this lifestyle modification. However, without a pre-existing base of regular exercise and when weighing more than normal, the advice was to progress very slowly. Most importantly, each month she needed to be slightly more active than the last. Initially just planning a regular walking regimen while using the stroller was considered sufficient, aiming for 3000–4000 steps per day, starting from a fortnight after returning home. After two months, this had increased to 6000 steps, and the patient added a ‘mums and bubs’ Pilates class twice per week, which she enjoyed. Her weight dropped to 79 kg, and she was encouraged to keep working on regular exercise to try to get back to pre-pregnancy weight, if possible, 6–8 months after birth.
Conclusion
Pelvic issues are a key consideration for women returning to exercise postpartum. This is particularly the case after Caesarean delivery or assisted vaginal delivery (eg forceps) where there is significant abdominal and/or pelvic trauma.
Development of musculoskeletal injuries is a significant risk in both lower and upper limbs. In the upper limb, wrist injuries are the most common, such as De Quervain’s tenosynovitis associated with extra loading due to changing, bathing and nursing. Ideally this would be prevented with some light but regular wrist strengthening and range-of-motion exercises in the antenatal period. Lower limb injuries, such as plantar heel pain, can occur because of a sudden increase in walking on return to exercise and with weight gain as an additional risk factor.
Weight loss (in a steady amount over months) is an additional challenge postpartum, as are the issues of support networks, which can assist with or hinder adequate return to exercise.
Key points
- An early return to exercise is safe and should be encouraged in the postpartum period.
- Pelvic floor exercise can be initiated in the immediate postpartum period.
- Consider nutritional screening and energy availability with breastfeeding.
- The body goes through many physical and hormonal changes during exercise; it is important to be patient, as it will take time to return to pre-pregnancy exercise levels.
Resources