Case
A man aged 30 years came to the clinic and presented with a two-week history of asymptomatic rash. The rash first appeared on the patient’s thighs and arms, and then involved the hands and trunk over the course of two weeks. The patient did not have any other remarkable discomfort or symptoms, such as fever, dizziness, headache, nausea, vomiting, or abdominal pain. He had a one-year history of hypertension that was well controlled with amlodipine 5 mg daily and a one-year history of hyperuricaemia. The patient had a family history of type 2 diabetes, with his mother having diabetes. The patient was obese, with a body mass index of 30 kg/m2.
Dermatological examination showed numerous yellow–red papules with erythematous halos symmetrically distributed on the extensor surfaces of his bilateral hands, arms and thighs (Figure 1A,B). Similar papules were scattered on the patient’s abdomen and flanks. The remaining physical examination was unremarkable. Dermoscopy of the skin lesions revealed pale yellow structureless areas, with arboriform telangiectasias and a surrounding erythematous brown halo (Figure 1C).
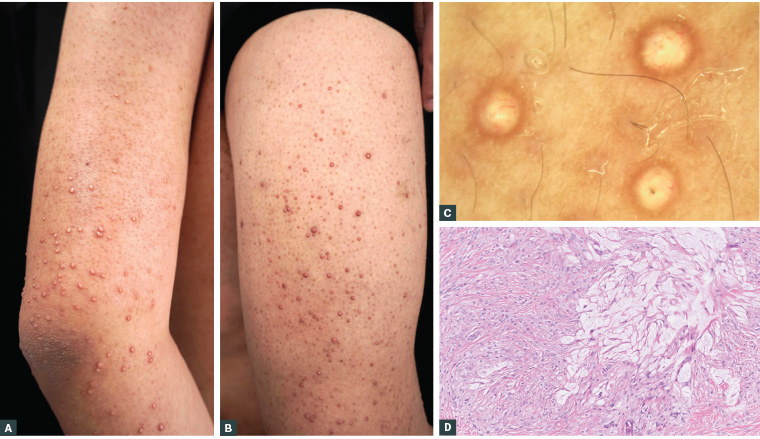
Figure 1. A, B. Numerous yellow–red papules with erythematous halos on the extensor surfaces of the arm and thigh. C. Pale yellow structureless areas with arboriform telangiectasias and a surrounding erythematous brown halo (dermoscopy; original magnification ×20). D. Histopathology revealed infiltration of foam cells into the dermis and extracellular loose lipids (haematoxylin and eosin stain; original magnification ×200).
Question 1
What is the most likely diagnosis and what are other possible differential diagnoses?
Question 2
How can the diagnosis be confirmed?
Answer 1
The most likely diagnosis is eruptive xanthoma, a subtype of xanthomas caused by localised deposition of lipids in the skin. Eruptive xanthoma is characterised by numerous distinctive yellow–red papules, with sudden onset, that are symmetrically distributed on the extensor surfaces of the extremities.1 Eruptive xanthoma can be asymptomatic or associated with pruritus, tenderness or a burning sensation. Importantly, eruptive xanthoma always develops in the context of systemic metabolic disorders, especially dyslipidaemias, such as severe hypertriglyceridaemia.
Other differential diagnoses include drug eruption, viral exanthem, generalised granuloma annulare and xanthogranuloma.
Answer 2
Serum lipid screening and a glucose test will help confirm the diagnosis. Eruptive xanthoma is not a simple dermatoses, but a significant indicator of systemic metabolic disorders.2 Severe hypertriglyceridaemia is considered the highest risk factor for the development of eruptive xanthoma, with approximately 8.5% of patients having triglyceride concentrations >20 mmol/L.2 Hypertriglyceridaemia can be caused by primary disease, mainly hereditary diseases like lipoprotein lipase deficiency, familial hypertriglyceridaemia and familial combined hyperlipidaemia. It also can result from secondary factors, including obesity, alcohol abuse, uncontrolled diabetes, hypothyroidism and some medications, such as systemic glucocorticoids, retinoids, cyclosporine, exogenous oestrogens and antiretroviral drugs.1,3 Therefore, in addition to the laboratory tests, a careful review of the patient’s medical history is needed to find the possible causes. Histopathology is not necessary and may be time consuming, but helps confirm the diagnosis and exclude other differential diagnoses. The accumulation of foam cells and extracellular lipid deposits are the key characteristics of eruptive xanthoma.2 In addition, doctors should be alert to the occurrence of possible concomitant conditions, such as acute hyperlipidaemic pancreatitis and diabetic ketoacidosis or hyperglycaemic hyperosmotic coma.
Case continued
A fasting blood sample from the patients was grossly lipaemic. Laboratory tests revealed fasting serum glucose 15.52 mmol/L (reference: 3.61–6.11 mmol/L), triglyceride 23.30 mmol/L (reference: 0.56–1.7 mmol/L), total cholesterol 12.53 mmol/L (reference: 3.4–5.2 mmol/L) and uric acid 545 µmol/L (reference: 150–420 µmol/L). The patient’s HbA1c was 9% (reference: 4–6%). A skin biopsy was performed, revealing the infiltration of foam cells into the dermis and extracellular loose lipids (Figure 1D). Based on the distinctive dermatological and pathological manifestations and concurrent severe hypertriglyceridaemia and diabetes, a diagnosis of eruptive xanthoma was made. Obesity and undiagnosed and untreated diabetes were considered to be the possible causative factors.
Question 3
How can this condition be managed?
Answer 3
The primary management is to control the dyslipidaemia and accompanying conditions. Along with diet and lifestyle modifications, systemic lipid-lowering drugs are usually administered, including statins, nicotinic acid, fibrates and bile acid sequestrants, with fibrates being the first-line treatment with significant triglyceride-lowering effects.4 The management of accompanying conditions, such as diabetes and pancreatitis, uses conventional treatments. The skin lesions of eruptive xanthoma usually resolve spontaneously with the treatment of the hypertriglyceridaemia.
Case continued
The patient was then referred to an internal medicine clinic. After systemic assessment, he was prescribed fenofibrate and pitavastatin to control hyperlipidaemia, and insulin and oral hypoglycaemic agents for his diabetes. After treatment for 1.5 months, the skin lesions subsided; after three months of treatment, total cholesterol was lowered within the normal range, triglyceride was 7.63 mmol/L, blood glucose was 9.56 mmol/L and HbA1c was 7.1%.
Question 4
What is the significance of this diagnosis?
Answer 4
As a skin manifestation of a systemic disorder, eruptive xanthoma gives clinicians an opportunity to determine potential accompanying comorbidities. Early recognition helps with prompt, effective management and prevents acute and chronic complications, including the progression of atherosclerosis, cardiovascular diseases and, in particular, acute severe pancreatitis, which can be fatal.
Key points
- Eruptive xanthoma is characterised by numerous yellow–red papules, with sudden onset, that are symmetrically distributed on the extensor surfaces of the extremities.
- Eruptive xanthoma is a significant indicator of systemic metabolic disorders, including dyslipidaemia and diabetes.
- Early recognition and prompt effective management help prevent acute and chronic complications.