To combat severe acute respiratory syndrome coronavirus 2 (SARS-Cov2), various approaches have been adopted internationally,1 leading to ongoing debate as to the most effective management strategy.2,3 Chinese authorities abolished the dynamic-zero approach on 7 December 2022.4 The authorities downgraded the COVID-19 virus into a second-level dangerous pathogen, abolished the zero-COVID policy and encouraged people to resume normal social activities. Moreover, the authorities encouraged the most vulnerable people to be vaccinated to boost their immunity and in an attempt to quickly reduce the number of acute infectious cases.5 As a result of these changes, over the following two months, 80% of the Chinese population were newly infected with COVID-19,6 probably facilitated by poor host immunity due to restrictive lockdowns over the previous three years. Vaccination rates at the time of change in the COVID-19 policy were >90% and 85% for the first and second doses, respectively,7 of the Sinopharm, Sinovac or CanSinoBio vaccines,8 excluding children aged <3 years.9
There are 200 general practitioners (GPs) in the Department of General Practice, Tongren Hospital, Shanghai, including affiliated GP clinics. These GPs serve approximately 99% of the 700,000 residents within the Changning district,10 with the hospital and affiliated clinics effectively being the only primary care system available to the residents. Following abolition of the zero-COVID policy, GPs were deeply uncertain about how the situation would unfold. At that time, 99% of the patients seen in the Department of General Practice were regular patients; <1% were new.
Prior to the policy change, the regular overall number of patients and the number of patients presenting with respiratory symptoms (mainly chronic obstructive pulmonary disease) was approximately 400 and 100/day, respectively, except on weekends (Figure 1A). To our surprise, following the abolition of the zero-COVID policy, the overall number of patients decreased by almost 50% between 15 and 25 December 2022. We believe this reduction in patient numbers was due to fear of SARS-CoV2 infection, with most residents whose condition was stable voluntarily staying at home and minimising the frequency of their visits.
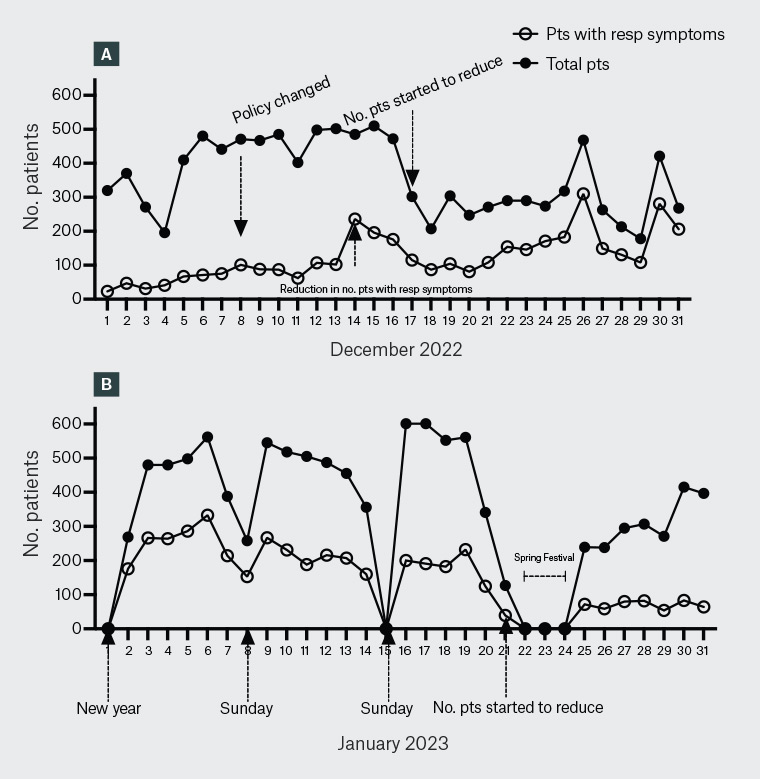
Figure 1. Daily numbers of total patients and patients with respiratory (resp) symptoms attending the Department of General Practice, Tongren Hospital, Shanghai, China, in (A) December 2022 and (B) January 2023.
Pts, patients.
Throughout China at this time, almost everyone was voluntarily wearing a mask to prevent virus transmission. However, despite this and the voluntary stay-at‑home approach, the number of patients with a respiratory infection increased more than three-fold by four days after the abolition of the zero-COVID policy (Figure 1). All patients with respiratory symptoms underwent chest X-ray/computed tomography and a full blood count, as well as a polymerase chain reaction (PCR) test for SARS-CoV-2 viral infection if they had not done a rapid antigen test (RAT). At this time (four days after the abolition of the zero-COVID policy), respiratory symptoms in >99% of patients were found to be due to COVID-19. These patients received symptomatic management, with elderly and/or immunocompromised patients also receiving nirmatrelvir/ritonavir (Pfizer, Shanghai, China). The main source of transmission of SARS-CoV2 was via family members as people continued with their everyday working lives.
Within the hospital and GP clinics, M95 masks and protective gowns were worn during consultations to protect staff. The windows were opened for one hour to allow fresh air into the rooms, and ultraviolet lights were used to irradiate the rooms before and after, but social distancing was abolished. Within the Department of General Practice, 95% of GPs and 100% of nurses were infected with COVID-19 in January 2023.
From 25 December 2022, the overall number of patients visiting the Department of General Practice returned to its previous level, including the usual drop in patient numbers on weekends. In contrast, the number of patients with respiratory symptoms remained at similarly high levels, with two peaks in patient numbers on 26 and 30 December 2022 that could not be clearly explained. Despite major holidays occurring during this time, most residents voluntarily stayed home in their regular residence; this is supported by reports of <5% occupancy rates of train carriages throughout Shanghai.11 The Department of General Practice usually manages regular patients with stable chronic conditions. Extremely sick patients were transferred to the in-patient department of Tongren Hospital. Notably, access to specialised COVID-19 hospitals was discontinued following the abolition of the zero-COVID policy.
There were no patient attendances at the Department of General Practice on New Year’s Day due to department closure (Figure 1B). However, the overall number of general practice patients gradually returned to previous levels throughout January 2023, possibly because of state-run education programs for residents over the preceding three-week period. In addition, by the end of January 2023, most of the community was COVID-19 positive (RAT self-testing). Free RAT kits were distributed by local councils to all residents in Shanghai.
The three decreases in the number of patient presentations on 8, 15 and 21 January 2023 were due to two weekends and the Chinese Spring Festival. No significant changes in patient numbers were observed afterwards. In contrast, the number of patients with respiratory symptoms remained high for most of January 2023, although this slowly tapered down towards 100 respiratory presentations by the end of January 2023. There were three decreases in the number of patient visits for respiratory symptoms (also on 8, 15 and 21 January).
It should be noted that this viewpoint presents simple observations from our Department of General Practice and has not incorporated the psychological/psychiatric impacts resulting from the sudden abolition of the zero-COVID policy.
In conclusion, as a result of the COVID-19 pandemic, our staff have had the opportunity to be trained and are prepared for any future pandemic, specifically in relation to staff personal protection, the handling of infectious patients and more effective and safe management of clinical practice in the event of a staff shortage.