Tropical North Queensland (NQ), Australia, has the highest global incidence of skin cancer.1 Management of skin cancer comprises a substantial proportion of general practitioner (GP) workload in Australia,2 and with limited access to specialist care due to a rural workforce shortage,3 this proportion is magnified in regional Queensland.
Baseline rates of surgical site infection (SSI) after skin excisions are high in rural NQ, possibly due to heat, humidity and rural lifestyle.4,5 SSI rates are also highest in complex flap and graft surgery6–8 below the knee.9,10 Despite this, Australian guidelines do not recommend antibiotic prophylaxis for this scenario,11 although international guidelines differ.12
Antibiotic resistance is a global health priority and resulted in 1.27 million deaths globally in 2019.13 Bacterial load reduction via full-body bathing with antimicrobial soap or antiseptic agent at least one day prior to surgery is strongly recommended by the Centers for Disease Control and Prevention (CDC) Guideline for the Prevention of Surgical Site Infection.14 Decolonisation of Staphylococcus aureus, commonly associated with SSI, using nasal mupirocin and chlorhexidine gluconate bathing preoperatively reduces the risk of SSI.15
Our choice of antibiotic prophylaxis considers antibiotic stewardship and uses the narrowest spectrum antibiotic to cover likely infecting microorganisms, guided by the microbiology of infections in previous studies and local data regarding resistance and sensitivities. Our previous studies have identified pansensitive S. aureus with only one Pseudomonas aeruginosa infection.16 Up to 22% of Staphylococcal infections in NQ are now methicillin-resistant S. aureus (MRSA), although this is more common with boils than SSI.17 Oral clindamycin is active against most Gram-positive cocci and community-acquired MRSA.10,18 Preoperative administration of intra-incisional clindamycin with local anaesthetic significantly reduces infection rates in Mohs micrographic surgery: 0.7% versus 2.4%.19–21 Our previous study using 2 g of cephalexin 30–60 minutes preoperatively in below-knee routine skin ellipse excision surgery decreased the infection rate from 35.7% to 12.5%.9 However, a similar study about below-knee complex flap and graft surgery showed a modest reduction and a negative trial (30.9–25.5%).
This trial aims to determine the efficacy of two interventions (oral clindamycin pre- and post-operatively; and preoperative chlorhexidine wash and nasal mupirocinin) in reducing SSI in people undergoing flap or graft procedures for treatment of skin cancer below the knee. This will be the first study to investigate both interventions as prophylaxis for SSI in complex skin surgery. If either intervention is successful, it will reduce patient morbidity while potentially reducing the use of oral antibiotics and associated adverse outcomes.
Methods
This study has been registered with the Australian New Zealand Clinical Trials Registry (ACTRN12624000076572).
Study design and setting
This randomised double-blinded, placebo-controlled trial will be conducted at three primary care skin cancer clinics in NQ. The study team have conducted several successful similar randomised controlled trials in this region.20,22,23 The data collection phase will occur over a nine-month period.
Participants and recruitment
Participants will be patients aged over 18 years presenting to recruiting clinics for surgical management of skin cancer below the knee that requires a complex surgical technique (flap or graft repair). Below-knee will be defined as below the lower pole of the patella anteriorly and lower border of the popliteal fossa posteriorly. Exclusion criteria will include allergy to clindamycin, chlorhexidine or mupirocin, existing skin infection, unable to provide informed consent, peripheral vascular disease, diabetes, current use of antibiotics, and clinical indication for antibiotic treatment following excision (eg valvular heart disease). Patients will be recruited by practice nurses/doctors who will receive formal training regarding appropriate consenting procedures. Eligible participants will provide written informed consent before entering the study.
Randomisation and intervention
Randomisation will be performed at the patient level with an allocation ratio of 1:1:1 to each treatment arm, stratified by clinic and surgeon. Randomised permuted blocks of four and six will be used. Treatment arms will be:
- Arm 1 – Bacterial load reduction: Patients will be screened nasally for S. aureus carriage seven to 10 days preoperatively. Those positive for S. aureus will receive nasal mupirocin ointment to be applied to the anterior nares nightly for three consecutive days preoperatively. All patients will use an all-over chlorhexidine body wash the night before and on the morning of the surgery and receive placebo antibiotics as per those is Arm 3 (Control) (Figure 1).
- Arm 2 – Clindamycin: Patients will be administered 450 mg of oral clindamycin 30–60 mins before surgery in the waiting room to enable monitoring for adverse reactions and an equal second dose at home six hours postsurgery. Participants will perform a placebo bacterial load reduction following the same protocol as in Arm 1 but will not be screened for S. aureus (Figure 1).
- Arm 3 – Control: This group represents normal standard of care in which no active bacterial load reduction (or nasal screening) or active clindamycin will be administered. Patients will receive placebo oral capsules (in lieu of clindamycin), placebo wash (in lieu of chlorhexidine) and placebo ointment (in lieu of nasal mupirocin). Placebo treatments will follow the same time schedule as their active counterparts in Arms 1 and 2 (Figure 1)
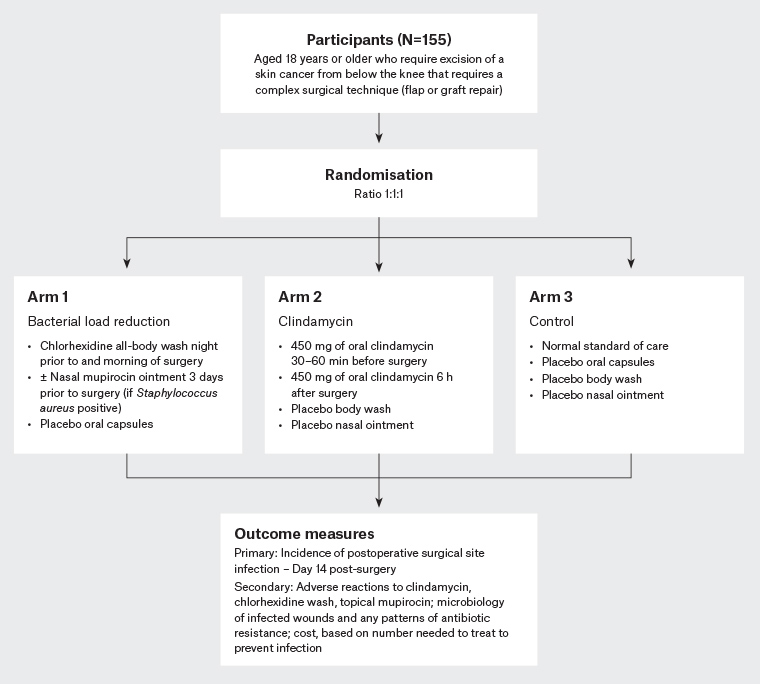
Figure 1. Protocol plan for the randomised double-blinded placebo-controlled trial. Click here to enlarge
Study procedure
A compounding pharmacist will prepare interventions for all three arms. Identical capsules will contain either 450 mg of clindamycin (Arm 2) or an inert powder vehicle for clindamycin (placebo treatment, Arms 1 and 3). Identical bottles will contain either chlorhexidine wash (chlorhexidine in saline) (Arm 1) or saline wash (Arms 2 and 3). Identical tubes will contain mupirocin nasal ointment (Arm 1) or soft white paraffin (vehicle for mupirocin nasal ointment) (Arms 2 and 3).
All intervention and placebo treatments will be uniquely coded using a sequence generated by a computer-generated random number table. Only the pharmacist will know the identity of the code. All clinic staff and patients will remain blinded to the allocation. Patients will be given a unique trial number corresponding to their allocation on enrolment.
Doctors will follow a strict surgical dressing and wound management protocol. The protocol, developed in consultation with participating staff, is modelled from similar trials9,10 and international guidelines.14 Drapes, gloves, sutures, skin antisepsis, local anaesthetic, dressings and postoperative wound care processes will be consistent across both sites. Patients will receive standardised verbal and written preoperative and postoperative instructions.
Data
Patient data will include age, gender, smoking status, diabetes, platelet modifiers (including aspirin and clopidogrel), anticoagulants and immunosuppressives (including prednisolone and methotrexate). Surgical data will include histology of the excised lesion, exact surgery site (using body site map), surgical repair technique, analgesia requirements and other complications (all adverse events). Data will be collected through use of spreadsheets completed by practice nurses and regularly audited by a member of the research team.
Outcome measures
The primary outcome measure is incidence of postoperative SSI. Patients’ wounds will be assessed for evidence of SSI when they present for removal of sutures (ROS) at day 14, or any time they present for wound review because of signs/symptoms of SSI, or opportunistically if they re-present for another reason. Ideally, wound assessment would be performed by a single outcome assessor at each practice; however, from a pragmatic perspective, several doctors/nurses will be available for assessments. There will be standardised in-house training regarding infection identification, to ensure validity and reliability. All wounds will be photographed following a standardised procedure (background, lighting and positioning) and assessed by a second blinded independent outcome assessor. Levels of agreement regarding infection/no infection will be measured using kappa statistic.
Patients with an SSI will be treated with antibiotics as clinically indicated. As per standard practice, all wounds with purulent discharge will be swabbed. A standardised follow-up telephone call of participants will be performed at 28 days to assess for delayed infection. Although patients will be instructed to present to their original treating clinic for ROS and wound assessment, standardised instructions will be provided should they need to follow up with a different GP (eg remote patients).
SSI will be determined in accordance with a modified version of the CDC definition for superficial SSI24 and includes:
- infection occurs within 30 days after excision, AND
- infection involves ONLY skin or subcutaneous tissue of the incision, AND
- at least ONE of the following:
- purulent drainage with or without laboratory confirmation from the superficial incision
- at least one of the following signs or symptoms: pain or tenderness, localised swelling, redness or heat
- diagnosis of superficial SSI by the GP
- stitch abscesses, characterised by minimal inflammation and discharge confined to points of suture penetration, will not be included as SSI.
Secondary outcome measures include:
- adverse reactions to clindamycin, chlorhexidine wash or topical mupirocin, manifesting as any of the following:
- anaphylaxis
- nausea, diarrhoea, vomiting
- skin irritation or contact dermatitis
- rash
- microbiology of infected wounds and patterns of antibiotic resistance
- cost, based on number needed to treat to prevent infection.
Data analysis
Demographic characteristics will be compared between groups at baseline. Chi-squared testing and multiple logistic regression will be used to compare the incidence of infection. Generalised linear models with random effects will be used to account for nesting by clinic and surgeon. The absolute risk difference, risk ratio and number needed to treat (to prevent one infection) will be calculated. All tests will be conducted at the 5% significance level.
Primary analysis will be by intention-to-treat with protocol violators analysed to the group they were originally allocated. As well as an additional per-protocol analysis, a sensitivity analysis will be conducted to model incidence of infection for lost-to-follow-up patients in three possible scenarios: (1) assuming all had SSI; (2) assuming all had no SSI; and (3) imputing data based on the rate of SSI in the allocated group.
Sample size
Sample size was calculated based on previous studies of SSI in NQ.20,22,23 Pooled analyses showed a weighted mean SSI rate of 25% as our predicted baseline infection rate.20,22,23 We decided an absolute reduction in the SSI rate of 20% (to 5%) would be clinically significant. To reach this conclusion with statistical confidence, a power more than 80% and a significance level of 0.05, a total of 49 patients would be required in each of the three groups (147 in total). Dropout rates in our previous trials have been less than 5%;9,20,22,23 therefore, an additional eight patients will be enrolled to counter potential attrition, providing a final sample size of 155.
Dissemination
Findings will be disseminated through conference presentations, journals and electronic media. A written lay summary of results will be displayed at participating clinics for the information of participants.
Ethical considerations
This project has been approved by the Queensland Health Human Research Ethics Committee (approval number 50257). We do not expect study interventions to place participants at any significant risk of harm, as we hypothesise a lower incidence of SSI in the intervention group, and the control group depicts normal standard of care. SSI is usually a minor, easily treated condition. To assure privacy and confidentiality, all data will be de-identified and spreadsheets and consent forms stored in a locked cabinet throughout the trial, and in a locked safe at trial conclusion for 15 years.
Discussion
Antibiotic resistance is a global health priority.25–30 Australia ranks seventh of 28 countries for antibiotic consumption, with more than twice the rate of the lowest prescribing Nordic countries,31 which have the lowest antimicrobial resistance rates.32
Development of resistance has a clear causal relationship with antibiotic consumption.33 With the innovative use of bacterial load reduction, our trial seeks to spare antibiotic prescribing and promote antibiotic stewardship, as well as reduce the SSI rate and therefore improve patient outcomes.
Strengths and limitations
The high throughput of surgery in our rural general practice setting means that the proposed trial is highly feasible, as proven by our previous studies.20,22,23 These have also shown patients’ willingness to participate in and complete trials; therefore, we believe recruitment of 155 patients is feasible. Our previous studies have also shown that SSI assessment at time of ROS facilitates a high follow-up rate.20,22,23
Although our study is conducted in a tropical rural setting, and our baseline infection rate is comparably high,7,8 we believe any relative risk reduction detected will be generalisable to other settings. Detection of a measurable decrease in SSI incidence with reduced bacterial load or oral clindamycin might result in changes in clinical practice. The findings of this pragmatic trial can potentially be immediately translated into clinical practice.