Background
Breast cancer is a significant cause of morbidity and mortality in Australia with one in seven women diagnosed in their lifetime, and one in 53 dying by age 85 years. Breast cancer screening is a vital tool in early detection but does not prevent cancer.
Objective
This article provides general practitioners (GPs) with evidence-based strategies for breast cancer prevention. It outlines breast cancer risk factors, personalised risk assessment tools, and the role of lifestyle modification, risk-reducing medication and risk-reducing surgery. Resources are included to assist GPs to educate, empower and support women to access prevention information.
Discussion
Population-level prevention targets modifiable risk factors, including obesity, alcohol use and physical inactivity. However, individual risk varies widely due to genetic and non-genetic factors, requiring a personalised approach. GPs play a key role in helping women understand their risk and make informed decisions about prevention options, aligned with their values.
Breast cancer is the most diagnosed cancer in Australian women, including in Aboriginal and Torres Strait Islander women, and the second leading cause of cancer deaths.1,2 Over 21,000 new breast cancer cases was predicted in 2024, with a growing incidence, including a 10% rise in people aged under 50 in the last 20 years.1,2 These statistics highlight the urgent need for prevention strategies.3
There are two complementary approaches to breast cancer prevention: population-level interventions aimed at minimising risk factors for all individuals; and identification of women with higher-than-average risk of breast cancer to offer personalised prevention interventions.3
General practitioners (GPs) play an essential role in cancer prevention and early detection.4,5 Australian research identified that 43.4% of cancer research priorities for primary care focus on prevention and early detection, particularly interventions targeting prevention strategies for breast, ovarian and colorectal cancer, as well as personal risk communication.6
The Australian Cancer Plan,7 the Aboriginal and Torres Strait Islander Cancer Plan8 and the Optimal care pathway for people with breast cancer9 support the need to proactively reduce cancer risk and for all Australians to be able to access personalised, evidence-based cancer prevention and early detection strategies. Figure 1 demonstrates Step 1 in the Optimal care pathway for people with breast cancer.9
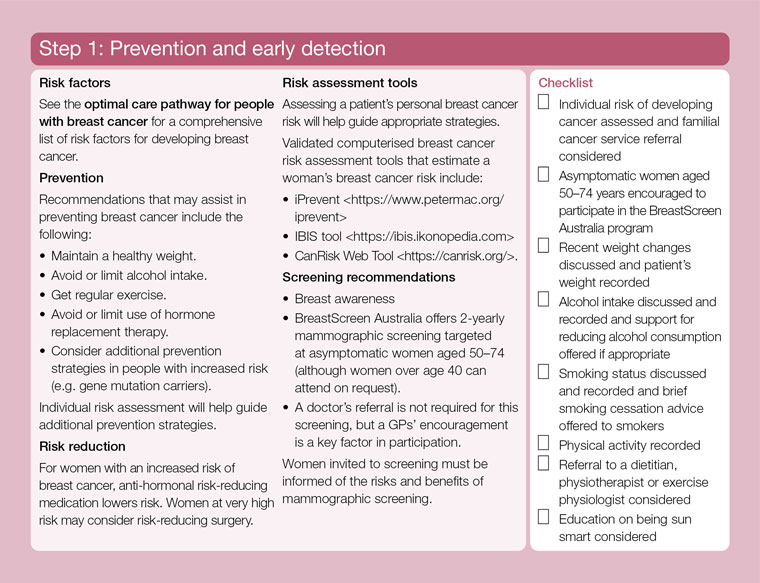
Figure 1. Optimal care pathway for people with breast cancer.9 Step 1: Prevention and early detection.
Reproduced with permission from Cancer Council Victoria and Department of Health Victoria. Optimal care pathway for people with breast cancer. 2nd edn. Vic: Cancer Council, 2021.
Breast awareness includes risk-factor awareness
Breast awareness – familiarity with the normal look and feel of one’s breasts – remains important for early detection, and women are recommended to promptly report any new or unusual change to their GP.10 While this has no impact on prevention, it provides an opportunity for GPs to educate women about risk factors for breast cancer and encourage risk assessment.
The strongest predictors of breast cancer risk are being female and increasing age, with more than 75% of cases occurring in women aged over 50.11 At least 5% of breast cancers are attributed to inherited genetic variants, primarily BRCA1 and BRCA2 mutations, which can be identified through genetic testing.12 Other genetic variants, such as PALB2, CHEK2 and ATM, may cause a modest increase in breast cancer risk,13 and clustering of low-penetrance single nucleotide polymorphisms (SNPs) in one individual, assessed as a polygenic risk score (PRS), can lead to higher risk.14
Other established risk factors include a family history of breast cancer, a history of radiation exposure (involving the breasts), non-invasive breast conditions such as atypical hyperplasia and lobular carcinoma in situ, a tall height and reproductive history (such as nulliparity and older age at first birth). Modifiable risk factors include alcohol consumption, having an elevated body mass index (BMI), physical inactivity, little or no breastfeeding in parous people, exogenous female hormone use and increased breast density.3,15
Modifiable risk factors such as post-menopausal overweight and obesity, alcohol consumption and physical inactivity contribute to around 21% of global breast cancer deaths.16 Up to 25% of breast cancers in high-income countries could be prevented by modifying risk factors.3 Table 1 shows the percentage of breast cancers attributable to modifiable risk factors.
The evidence regarding smoking as a risk factor for breast cancer is less convincing – but generally consistent in showing a positive association between current or former tobacco smoking versus never smoking.17
Breast (or mammographic) density is the proportion of fibroglandular tissue in the breast as measured on a mammogram. Breast density is typically listed as a non-modifiable risk factor but can be reduced with medication.18 The approximately 12% of Australian women with extremely dense breasts19 are 4–6 times more likely to get breast cancer than those with fatty breasts,20 and are more likely (4.4/1000 compared to 0.7/1000 for fatty breasts) to develop larger, more advanced cancer in between routine screenings (interval cancers).21 Over 70% of breast cancers occur in women with dense breasts,22 who also have almost a two-fold increased risk of developing a contralateral breast cancer.23
| Table 1. Percentage of breast cancers attributable to modifiable risk factors |
| Risk factor |
Percentage of breast cancers attributable |
| Obesity |
8–13%16,24 |
| Alcohol |
8–16%24,25 |
| Physical inactivity |
2–10%16 |
| Not breastfeeding |
4.7%24 |
Hormone use:
- Menopausal hormone therapy
- Hormonal contraceptive use
|
2.1%26
0.8%26 |
Risk assessment tools for personalised prevention
The first step in personalised breast cancer prevention is risk assessment. Proactive risk assessments beginning at age 25–30 years are required to facilitate identification of, and preventive interventions for, those who are at high risk of early-onset breast cancer.3 Risk assessment should continue at intervals throughout a woman’s life, for example every 10 years to account for changing risk factors and advances in medical knowledge that might inform the risk assessment.3 A potential time point for a comprehensive risk assessment could be at age 40 years, or when an individual has decided that they do not want any or more children, in which case risk-reducing medication such as tamoxifen could be considered.3
Risk assessment tools available in Australia are iPrevent,27 CanRisk (BOADICEA v7)28 and IBIS (Tyrer-Cuzick v8).29 CanRisk is designed for use by healthcare professionals to help them communicate and discuss breast and ovarian cancer risk with their patients. IBIS/Tyrer Cuzick calculates breast cancer risk by combining familial risk with classic risk factors, with the latest version (v8) incorporating mammographic density. Tyrer-Cuzick v8 or later is considered the ‘clinically relevant evaluation algorithm’ for risk estimation to support the MRI Medicare rebate (MBS item 63464) eligibility for patients at high risk of developing breast cancer.30
iPrevent, developed in Australia, is recommended by Cancer Australia, and is a clinical resource accepted by The Royal Australian College of General Practitioners (RACGP). It can be completed online by women and/or their GPs to facilitate prevention and screening discussions. Focus groups of consumers and familial cancer clinicians (FCCs) support its use.31 iPrevent presents risk information as a statistic, a pictogram and a graph to account for different preferences for receiving risk information. It is the only tool that also presents screening and prevention options appropriate to the estimated risk, based on Australian guidance.32
Evidence-based risk management recommendations
Current evidence-based guidelines for the prevention of breast cancer are lacking. The NSW Cancer Institute’s eviQ guidelines provide risk management protocols, as outlined in Table 2, for women at moderately increased risk33 (based on family history) and for those at high risk – with, and with no family history of ovarian cancer.34,35
| Table 2. eviQ risk management protocols according to risk category33–35 |
| Risk category |
Lifestyle modification |
Risk-reducing medication |
Risk-reducing surgery |
Average risk
(<1.5x population risk; 11% LTR) |
✅ |
Not recommended |
Not recommended |
Moderate risk
(1.5–3x population risk; ≥17% but <30% LTR) |
✅ |
Consider use of medication to reduce risk of developing breast cancer:A
- Pre-menopausal ≥35 – consider tamoxifen
- Post-menopausal – consider raloxifene, aromatase inhibitors or tamoxifen
|
Generally not recommended |
High risk
(>3x population risk; ≥30% LTR) |
✅ |
Consider use of medication to reduce risk of developing breast cancer:A
- Pre-menopausal ≥35 – consider tamoxifen
- Post-menopausal – consider raloxifene, aromatase inhibitors or tamoxifen
|
Discuss bilateral risk-reducing mastectomy |
| ARequires assessment of risks and benefits for an individual. Refer to COSA guideline for medications to lower the risk of breast cancer – Clinician guide.38 |
| LTR, lifetime risk. |
Lifestyle modifications
Community awareness about modifiable risk factors for breast cancer remains low in many countries. Although educational interventions can increase knowledge about risk factors, this alone is not generally sufficient for sustained behavioural change.3 Despite this, evidence suggests that adhering to guidelines on weight control, physical activity, alcohol intake and diet can significantly reduce breast cancer risk. For example, women who followed the American Cancer Society’s recommendations saw a 22–31% lower risk of developing breast cancer compared to those who were less adherent.36,37
Risk-reducing medication – chemoprophylaxis or chemoprevention
Risk-reducing medication can decrease breast cancer risk by 30–60%.38 It is an efficacious breast cancer prevention option for high-risk women who do not wish to undergo (or who wish to postpone) risk-reducing mastectomy. It is under-utilised in Australia, with only 1.4% of kConFab women study participants at increased risk of breast cancer reporting use.39 Over 50% of these women, two (3%) breast surgeons, and 51 (35%) family physicians were not aware of chemoprevention. Barriers for use for women and clinicians included lack of information and side effects.39
There are two main categories: selective estrogen receptor modulators (SERMs) – tamoxifen and raloxifene; and aromatase inhibitors (AIs) – anastrozole and exemestane. Tamoxifen is suitable for both pre-menopausal (but not when trying to conceive, pregnant or breastfeeding) and post-menopausal women, while raloxifene is only for post-menopausal women.39
These medications only reduce the risk of hormone receptor-positive breast cancer, but this is the most common breast cancer phenotype and the one that is increasing in incidence.39
Tamoxifen and, to a lesser extent, raloxifene, increase the risk of thromboembolic disease. Tamoxifen increases the risk of endometrial cancer. Common side effects of tamoxifen are vasomotor symptoms, and vaginal discharge and dryness.38,39 Common side effects with raloxifene are leg cramps and vasomotor symptoms.38,39
Expected frequency trees, developed for a hypothetical Australian population of women at moderate risk of breast cancer (relative risk 1.8) are available to demonstrate outcomes of taking raloxifene or tamoxifen for five years, when compared with no treatment.40
Strategies to manage side effects include swapping to a different agent in post-menopausal women or modification of tamoxifen dose. Ten-year data shows tamoxifen 5 mg once daily for three years significantly prevents recurrence from non-invasive breast cancer after seven years from treatment cessation, without long-term adverse events.41
Referral to a specialised service, such as the Preventing Cancer with Medications (PCMed) Service at the Peter MacCallum Cancer Centre is an option.
Risk-reducing surgery – preventive or prophylactic mastectomy
Risk-reducing surgery, including bilateral mastectomy, is an option for women at very high risk of developing breast cancer, particularly those with significant family history or known genetic mutations such as BRCA1 or BRCA2.34,35 Bilateral mastectomy is associated with a more than 90% decreased risk of breast cancer in observational studies.42
High-risk women should be empowered to make their own informed decision, considering their individual risk and health status, personal values, life circumstance, and the potential benefits and risks of surgery. The role of breast reconstruction and options available should be discussed with those considering risk-reducing mastectomy.
Research
The prevention of hormone receptor-negative breast cancer remains an area of unmet need. Ongoing trials, such as the BRCA-P study, are investigating the use of denosumab, a RANK ligand inhibitor, to prevent hormone receptor-negative breast cancer in BRACA1 mutation carriers.43 Early pre-clinical studies showed that inhibiting the RANK pathway significantly reduces the proliferation of cancer-prone cells.43
Other novel prevention strategies being researched include medications that target molecular pro-survival signals, medications that mimic the breast cancer protection mechanisms from pregnancy and lactation, and vaccines that stimulate the immune system to recognise and destroy pre-cancerous or cancerous cells.3
Putting prevention into practice
General practice consultations offer numerous opportunities to discuss breast health, including awareness, cancer risk factors and risk-reduction strategies. Reproductive health encounters provide a natural entry point to start these conversations. Subsequent consultations can build on this by assessing modifiable risk factors and exploring options to address areas of concern. Routine risk assessments can begin at age 25–30 years and be revisited at key milestones, such as age 40 years, when free screening is available through BreastScreen Australia. Perimenopause or menopause is another key timeframe to reassess risk, encourage preventive lifestyle choices and reinforce the role of screening in early detection. Follow-up appointments after screening assessments with benign results also present valuable moments to revisit risk awareness and prevention. GPs, patients and the public have access to numerous resources to assist at all stages of risk assessment and management, as detailed in Tables 3 and 4.
Conclusion
Breast cancer prevention requires both population-wide and personalised approaches, combining lifestyle modifications with targeted interventions for those at moderate and high risk. General practitioners play a critical role in guiding women through risk assessment and prevention strategies, including risk-reducing medication and surgery. By discussing risk factors, evaluating overall risk, outlining the benefits and risks of interventions, and referring where appropriate, GPs can support informed decision-making, allowing women to choose options aligned with their values and circumstances.
Key points
- Breast cancer screening does not prevent cancer.
- Breast cancer risk is multifactorial and should be assessed using a validated tool that incorporates genetic and non-genetic factors.
- Breast cancer risk assessment should be undertaken at regular intervals.
- Medical and surgical interventions can reduce risk in women who have a moderate to high risk of developing breast cancer.
- GPs can assist with personalised risk assessment and implementation of risk-reducing strategies.