Alcohol use causes a high disease burden and has significant social and economic consequences.1,2 Although alcohol can be consumed in line with low-risk consumption guidelines,3 excess consumption and other risk factors can lead to medical complications.4 Alcohol dependence is characterised by a strong internal drive to use alcohol, manifested by an impaired ability to control use, with increasing priority given to use despite harm and negative consequences.5 Alcohol consumption in excess is also known to negatively affect nutritional status, but this might be less recognisable in the early stages of risky drinking.6 ‘Risky’ drinking is defined as more than 10 standard drinks a week and more than four standard drinks in one day.3 General practitioners (GPs) play an important role in screening alcohol consumption and engaging patients in discussions about alcohol and nutrition.7
Alcohol provides little beyond energy (29 kJ/g) to dietary intake and, when consumed in addition to other foods and fluids, promotes a positive energy balance.8 A standard drink contains 10 g of alcohol; this equates to 290 kJ. However, this might translate to 435 kJ in a 150-mL glass of wine, and might further depend on the types of mixers used, such as soft drinks or juice. This is visually represented in Figure 1.
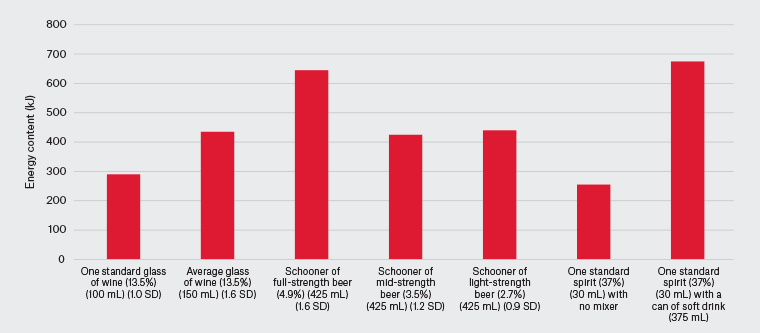
Figure 1. Comparison of the average energy content in kilojoules (kJ) of alcoholic beverages. Click here to enlarge
SD, standard drink.
However, alcohol’s influence on promoting weight gain and obesity is variable.8 This can be related to other factors such as gender, sleeping habits and physical activity levels. Alcohol consumption also affects energy metabolism. Although risky drinkers more consistently gain weight and are more likely to have a body mass index (BMI) above the healthy range, paradoxically, those with high levels of alcohol intake lose weight.8 In some instances, patients might prioritise alcohol consumption over other food or fluids, resulting in caloric intake without nutrient intake. Those with a hypermetabolic state (eg advanced liver disease or acute pancreatitis) might present with weight loss if oral intake is not sufficient to meet increased metabolic demands. Initially, patients might present with a healthy BMI but, over time, with insufficient oral intake and weight loss, present as underweight.
Malnutrition can involve a deficiency, excess or imbalance of nutrients, resulting in adverse effects on body composition, function and health outcomes.9 Most commonly, this is through inadequate consumption of food and fluids. Malnutrition can occur at all body sizes, including in those who might have a healthy BMI.10 In a cohort of patients admitted to hospital for alcohol withdrawal, 88% of patients presented with a BMI >20 kg/m2, but one in two patients were identified as being at a medium to high risk of malnutrition.11 Alcohol increases the risk of malnutrition, with 20% of patients with well-compensated liver disease and more than 60% of patients with advanced cirrhosis being malnourished.12 There is limited literature reporting on rates of malnutrition in patients in the absence of advanced liver disease.11 This emphasises the need for routine screening for malnutrition in patients who drink at risky levels.9,10
Alcohol has a significant effect on the digestion, absorption and metabolism of nutrients, which can lead to micronutrient deficiency and the development of chronic disease.13 Micronutrients are vitamins and minerals needed by the body to maintain normal body function. Over half the patients admitted to hospital for substance use treatment, including alcohol, are deficient in vitamins, minerals or electrolytes.14,15 This includes deficiencies in vitamin C, vitamin A and iron. Nutritional deficiencies are common and are major contributors to the morbidity related to alcohol use (eg thiamine deficiency causing Wernicke–Korsakoff syndrome).16 There is an absence of best-practice guidelines to support GPs in the management of malnutrition and nutritional deficiency in this patient group.
Aim
This article reviews some of the nutritional considerations in patients who drink at risky levels or who have alcohol use disorder (AUD), with the aim of enhancing GPs’ awareness of the nutritional considerations in this patient group.
Alcohol use assessment
Screening for alcohol risk can be conducted opportunistically, during presentations for potentially alcohol-related conditions or during routine preventive health assessments.17 Screening for alcohol risk using the Alcohol Use Disorders Identification Test–Concise (AUDIT-C) can help GPs identify patients who drink at risky levels or have AUD. AUDIT-C scores of ≥4 for men and ≥3 for women should trigger a more detailed review.18 Following screening, GPs are able to deliver advice on lower-risk alcohol consumption levels, deliver brief interventions and consider referring to multidisciplinary team members as required.
Nutrition assessment and management
Nutrition risk screening is a simple and first step to identify patients at risk of malnutrition.19 Measurement of BMI and/or waist circumference and a brief assessment of dietary intake are recommended for all Australians as part of routine preventive care every 6–24 months depending on risk level.17 As part of taking a social history, GPs might be aware of other social and environmental conditions that could affect an individual’s health and nutrition. This might include issues such as their ability to access or store food, known as food insecurity,20 and could be due to financial concerns, the prioritisation of purchasing alcohol over food or homelessness.
Malnutrition
GPs routinely record waist circumference, height and weight and calculate BMI. These tools can help identify whether a patient is within a healthy weight range or has lost weight between GP visits. The Malnutrition Universal Screening Tool (MUST), which includes measures of BMI and unplanned weight loss in the past three to six months, has been recommended for use in ambulatory settings.21 For patients who are identified at high risk of malnutrition using MUST (ie a score of ≥2), GPs can consider referral to an Accredited Practising Dietitian (APD) for comprehensive nutrition assessment.19,22 However, weight loss might not be obvious and might be masked by the presence of fluid retention, including oedema and ascites. Mid-upper arm circumference can be used as a substitute for assessing BMI in patients who are difficult to weigh or have other factors that might influence weight, such as fluid retention.22 Table 1 summarises the variables and considerations when using MUST.
| Table 1. Measures of the Malnutrition Universal Screening Tool (MUST)22 |
| Variable |
Frequency |
Considerations |
| Height (cm) |
|
- If unable to measure height, consider estimation using ulna length
|
| Weight (kg) |
Routinely at each clinic visit |
- Remove baggy clothes
- Examine for oedema or ascites
- Examine for muscle or fat wasting
|
| BMI (kg/m2) |
Routinely at each clinic visit |
- Consider referral to a dietitian if underweight (BMI <18.5 kg/m2) or BMI <23 kg/m2 for >65 years
- Consider use of MUAC to estimate BMI in the presence of fluid retention
|
| Weight loss (%) |
Routinely at each clinic visit |
- Consider time and rate of weight loss
- Consider referral to dietitian if weight loss >5%
|
| BMI, body mass index; MUAC, mid-upper arm circumference. |
Pathology testing
The prevalence of micronutrient deficiencies increases with increasing alcohol consumption.23 Existing guidelines have highlighted that there are several micronutrient deficiencies that are common to alcohol dependence.23 Micronutrient concentrations should be interpreted in the context of the clinical assessment and the acute phase response. For example, ferritin is an acute phase protein and, when elevated, might mask underlying iron deficiency.23 Therefore, micronutrient status should be assessed alongside C-reactive protein and albumin.23 Investigations should be ‘chosen wisely’ according to clinical presentation to ensure testing is rational.24 Table 2 provides suggested pathology testing, findings and associated physical signs, symptoms and outcomes.
| Table 2. Pathology tests and physical signs, symptoms and outcomes25 |
| Pathology test |
Finding |
Physical signs, symptoms and outcome |
Triglycerides
Cholesterol |
- Elevated triglycerides
- Elevated cholesterol
|
- Cardiovascular disease
- Cerebrovascular disease
|
| Full blood count |
- Megaloblastic anaemia
- Thrombocytopenia
|
- Gastrointestinal disturbance
- Tiredness
- Bleeding
|
| Albumin |
|
- Chronic weakness or fatigue
- Ascites, localised oedema
|
| Thiamine |
- Low thiamine (not routinely measured)
|
- Neurological symptoms
- Ataxia
- Wernicke–Korsakoff syndrome
- Dementia
|
| Vitamin D |
|
- Osteopenia/osteoporosis
- Depression
|
| Iron |
- Elevated ferritin in advanced liver disease/cirrhosis
- Low iron, ferritin in advanced liver disease with bleeding varices
|
|
| Folate |
- Low folate
- Megaloblastic anaemia
|
- Neuropsychiatric symptoms
- Tiredness
- Mouth ulcers or inflammation
|
| Vitamin B12 |
|
- Peripheral neuropathy
- Neuropsychiatric symptoms
- Weakness or fatigue
- Memory impairment or confusion
|
| Liver function tests |
- Elevated GGT (early)
- Global elevation (late)
|
- CirrhosisA
- Jaundice
- Elevated risk of HCC
|
| Magnesium |
|
|
| Vitamin KB |
|
|
| Coagulation studies |
- Elevated APTT
- Elevated INR
|
|
| HbA1c |
|
|
| Lipase |
|
- Pancreatitis
- Malabsorption
|
AUltrasound/elastography might also play a role in assessing the extent of cirrhosis.
BNot covered by a Medicare rebate.
APTT, activated partial thromboplastin time; GGT, gamma-glutamyl transferase; HbA1c, glycated haemoglobin; HCC, hepatocellular carcinoma; INR, international normalised ratio of prothrombin time. |
Nutrient supplementation and education
There is variable literature on nutrient supplementation in the context of patients who drink at risky levels or have alcohol dependence.26,27 However, vitamin and mineral supplementation should be commenced to treat confirmed or clinically suspected deficiency.23 One nutrient of importance is thiamine, given the established evidence of its efficacy in the treatment and prevention of Wernicke encephalopathy.1
Thiamine 100 mg orally should be considered for all patients who drink alcohol at risky levels.1 In healthy patients who drink at risky levels but have a good dietary intake, oral thiamine 300 mg should be administered for three to five days.1 However, in those patients with poor dietary intake and generally poor nutritional status, parenteral thiamine 300 mg (intravenous if hospitalised) should be administered for several days, with subsequent oral doses of thiamine 300 mg daily for several weeks.1 Oral supplementation of thiamine 100 mg daily should continue indefinitely in an alcohol-dependent patient who continues to drink alcohol.1
For all, a healthy, balanced diet is the priority (ie not replacing healthy food with alcohol). However, a multivitamin might be recommended for those unable to achieve a balanced diet. Specific nutritional deficiencies identified on pathology might also need replacement (eg magnesium). Other harm-minimisation strategies might be discussed with patients to address alcohol-related behaviours.1 This can include strategies such as alternating alcohol with non-alcoholic drinks and eating before drinking. When drinking socially, it might also include ordering small serves and distracting yourself while drinking, such as by talking to friends or playing pool.
Some, but not all, nutritional supplements are available on the Pharmaceutical Benefits Scheme, including thiamine and magnesium for Aboriginal people at risk.28 Those who are referred to an APD might be eligible for oral nutrition supplements (eg high-energy and high-protein ‘sip supplements’) through the home enteral nutrition program. Those with access to the National Disability Insurance Scheme (NDIS) might be eligible for nutritional supplements and the services of an APD.
Multidisciplinary team and nutritional care coordination
Multidisciplinary team collaboration is essential in supporting nutritional interventions. There is established evidence that multidisciplinary teams including dietitians contribute to improved patient outcomes for alcohol-related liver disease.29 For example, patients identified at risk of malnutrition using MUST could be referred to an APD for a comprehensive nutrition assessment and intervention. Similarly, patients identified to have difficulty accessing food and fluids might be referred to non-governmental organisations that provide or facilitate access to food. The use of chronic disease management plans and team care arrangements, or mental health care plans, might facilitate referral and access to these services, promoting disease prevention and independence and improving quality of life.30 Access to multidisciplinary team supports for eligible patients might also be achieved through the NDIS. Table 3 summarises potential multidisciplinary team members and their roles.
| Table 3. Multidisciplinary team members and their roles to support nutrition interventions |
| Team member |
Potential roles |
| Drug and alcohol team |
- Harm-minimisation strategies and counselling
- Treatments including medication, withdrawal services or residential rehabilitation
- Specialist services for vulnerable population groups
|
| APD |
- Comprehensive nutrition assessment and nutrition counselling
- Diagnosis and treatment of malnutrition
- Nutrition supplementation and access to HEN services
|
| Social worker |
- Comprehensive psychosocial assessment and case management for individuals and/or families
- Risk assessment and therapeutic interventions for chronic health conditions (eg mental health and trauma)
- Referral and advocacy to other services for additional support (eg housing support, financial support, food access, aged package, NDIA)
|
| Occupational therapist |
- Development of life skills and support re-engagement with routine
- Functional assessment or home assessment in those with severe AUD
- Provide advice and support access to aged care packages and NDIA
|
| Liver clinic |
- Specialist nurse-led services for cirrhosis management
- Specialist allied health services, such as gastroenterological dietitian
- Gastroenterologist review for cirrhosis, ascites, gastroscopy, treatment of varices
|
| Mental health team |
- Specialist mental health services including a clinical psychologist or psychiatrist for short-term (eg crisis) and long-term support options
- Case management
- Specialist services for vulnerable populations
|
| Other |
- Services and NGOs that support access to food, such as food banks, including organisations such as OzHarvest and Foodbank
- Services and NGOs that support access to safe accommodation, such as Mission Australia
|
| APD, accredited practising dietitian; AUD, alcohol use disorder; HEN, Home Enteral Nutrition; NDIA, National Disability Insurance Agency; NGOs, non-governmental organisations. |
Case study: John
John, aged 45 years, presents to your general practice for a laceration following a fall on the weekend. The practice nurse has conducted screening for smoking and alcohol as part of quality improvement activities, and has completed a set of observations. John consumes three standard drinks five days a week and has a couple of ‘big nights’ with workmates each weekend, with an AUDIT-C score of 8. He has never had any seizures or tremors as symptoms of withdrawal. You discuss harm minimisation with John, discussing a reduction in alcohol intake, which is his preferred option, rather than immediate cessation, as well as the option of referral to a drug and alcohol counsellor.
As part of your routine consultation, you collect John’s height and weight to calculate his BMI. You ask John to remove his clothing, which appears to be loose fitting around his arms and legs, although John has a small belly. John weighs 60.0 kg and is 178.0 cm tall; his BMI is 18.9 kg/m2 (normal 18.5–24.9 kg/m2). You notice visual muscle wasting in his calf. John reports he has unintentionally lost 5 kg in the past four months (7.7%). On discussion, John reveals he has separated from his partner and moved out, and has been living off takeaway food. A symptom review and physical examination does not suggest cancer as a cause. You calculate John’s overall risk of malnutrition and identify him as high risk. You consider ordering blood tests, as well as urinalysis and faecal occult blood testing because of the weight loss. You recommend oral thiamine 300 mg for three to five days and then thiamine 100 mg thereafter.
John returns to the clinic following his blood test. The blood results show that John has macrocytosis on full blood count, raised gamma-glutamyl transferase and high triglycerides. You consider John’s eligibility for a chronic disease management plan and team care arrangement for enhanced primary care referral to an APD. You consider referral to a psychologist or other relevant healthcare professionals identified in Table 3.
Conclusion
The nutritional considerations in patients who drink at risky levels or who have alcohol dependence extend beyond the evaluation of BMI alone because patients who have a healthy BMI might also be malnourished. Consideration should be made around recent weight loss, signs of fat or muscle wasting and suspected or confirmed nutritional deficiency through pathology testing. Referral to members of the multidisciplinary team should be considered to support and address barriers related to nutrition and to provide treatment and support to patients and families, translating to improved health and nutrition outcomes.
Key points
- Ask patients about alcohol use and screen for alcohol use using the AUDIT-C.
- Ask patients about their dietary intake, routinely record weight and calculate BMI. Routinely assess risk of malnutrition and consider referral to members of the multidisciplinary team, such as an APD, to address nutritional concerns.
- Encourage a balanced diet and a reduction in alcohol use, and supplement for confirmed or suspected micronutrient deficiency.
- Thiamine supplementation should be provided to all patients undergoing alcohol withdrawal, with long-term supplementation considered for those who continue to drink.
- For patients with alcohol dependence or AUD, consider referral to a multidisciplinary alcohol and other drugs team.